Downloaded 53 times

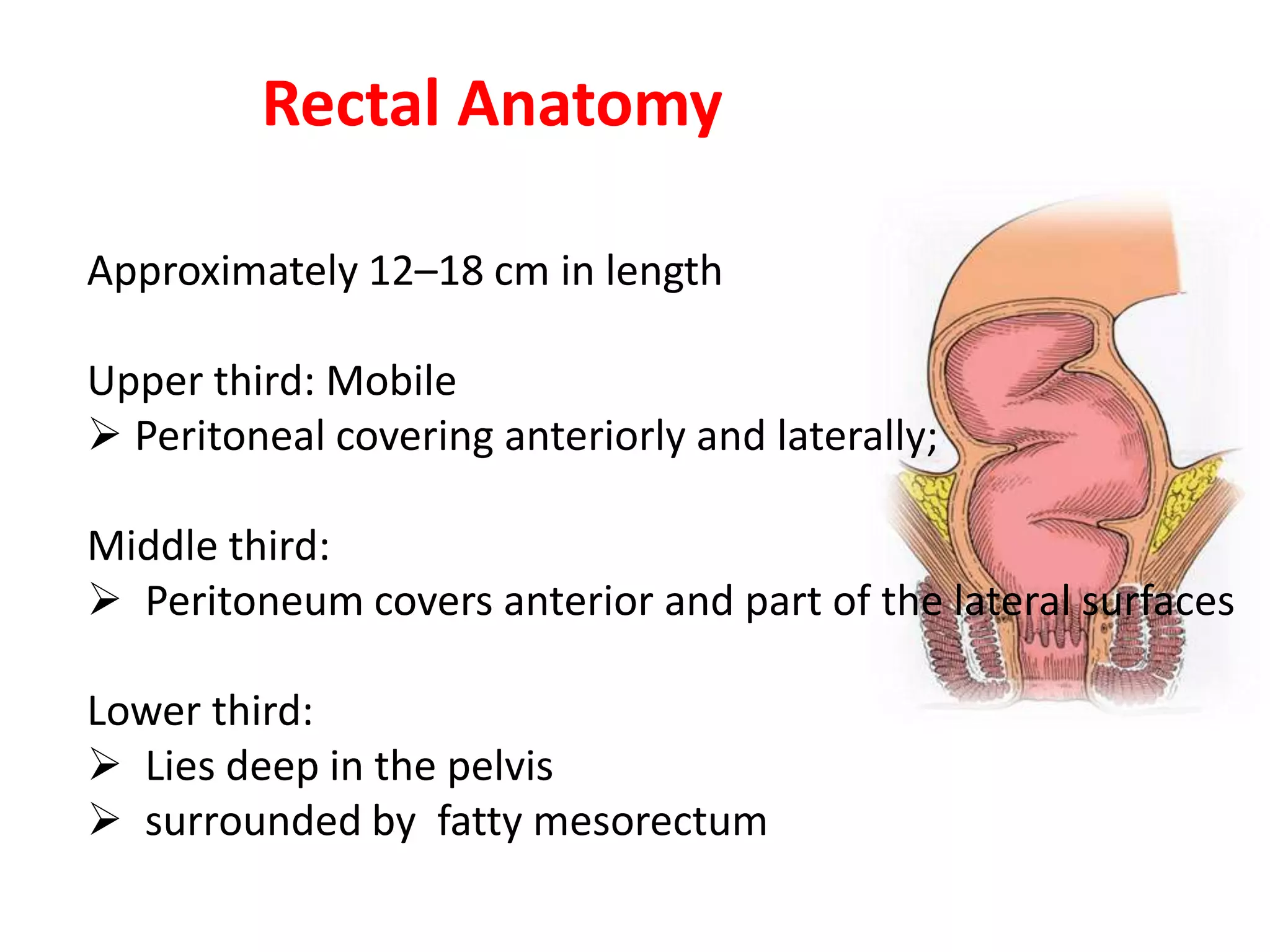






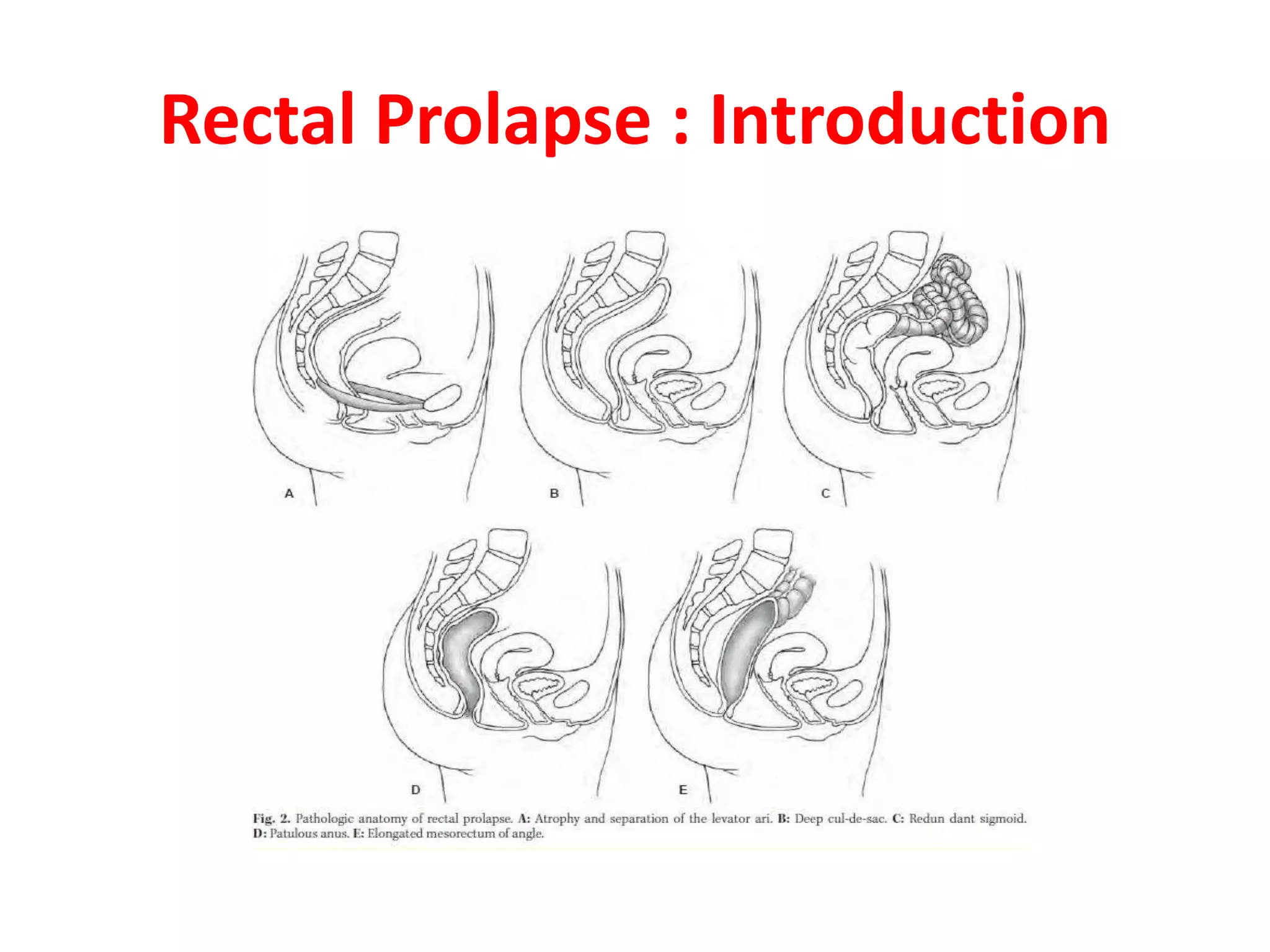








































This document provides information about rectal prolapse including its anatomy, causes, clinical presentation, and surgical treatment options. It begins with a description of the rectal anatomy including its blood supply, lymphatic drainage, and curves. It then discusses the causes and types of rectal prolapse and explains how factors like pelvic floor weakness can lead to its development. Common signs and symptoms are outlined. Both perineal and abdominal surgical approaches are described in detail including the Thiersch, Delorme, Altemeier, and Wells procedures. Postoperative care is also reviewed. The document provides a comprehensive overview of rectal prolapse.










































































