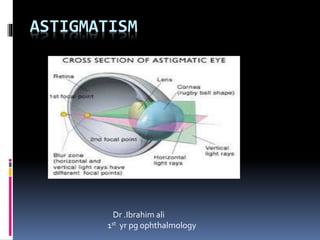
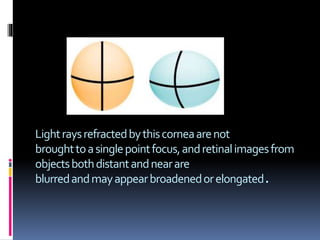
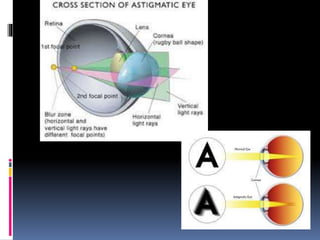
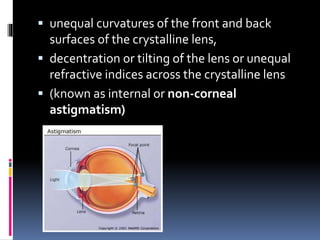
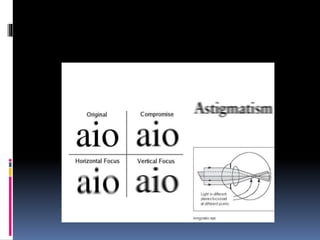
Astigmatism occurs when the cornea is not uniformly curved, causing light rays to not converge at a single focal point and resulting in blurred vision. It is most often caused by an uneven curvature of the cornea (corneal astigmatism). Symptoms include distorted or blurred vision at all distances. Astigmatism is commonly measured using a keratometer and can be corrected using spectacle lenses, contact lenses, or refractive surgery. Prescribing cylinders for spectacle correction requires determining the axis of astigmatism and cylinder power through retinoscopy techniques.