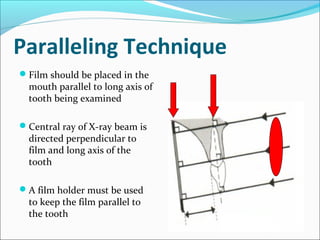
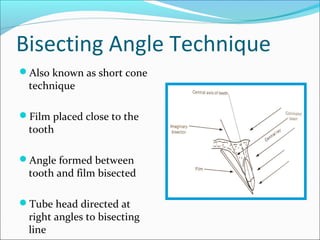
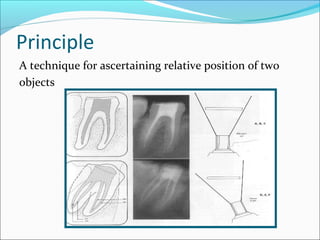
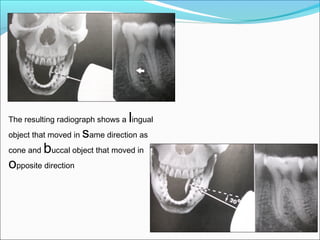
This document discusses dental radiography and x-rays. It defines key terms like radiograph and radiology. It describes the components of a dental x-ray unit and different types of radiographs like bitewings and panoramic x-rays. It discusses techniques like paralleling, bisecting angle technique and SLOB technique. It also covers topics like indications for radiographs, radiation safety, and advantages and disadvantages of digital radiography compared to conventional film.