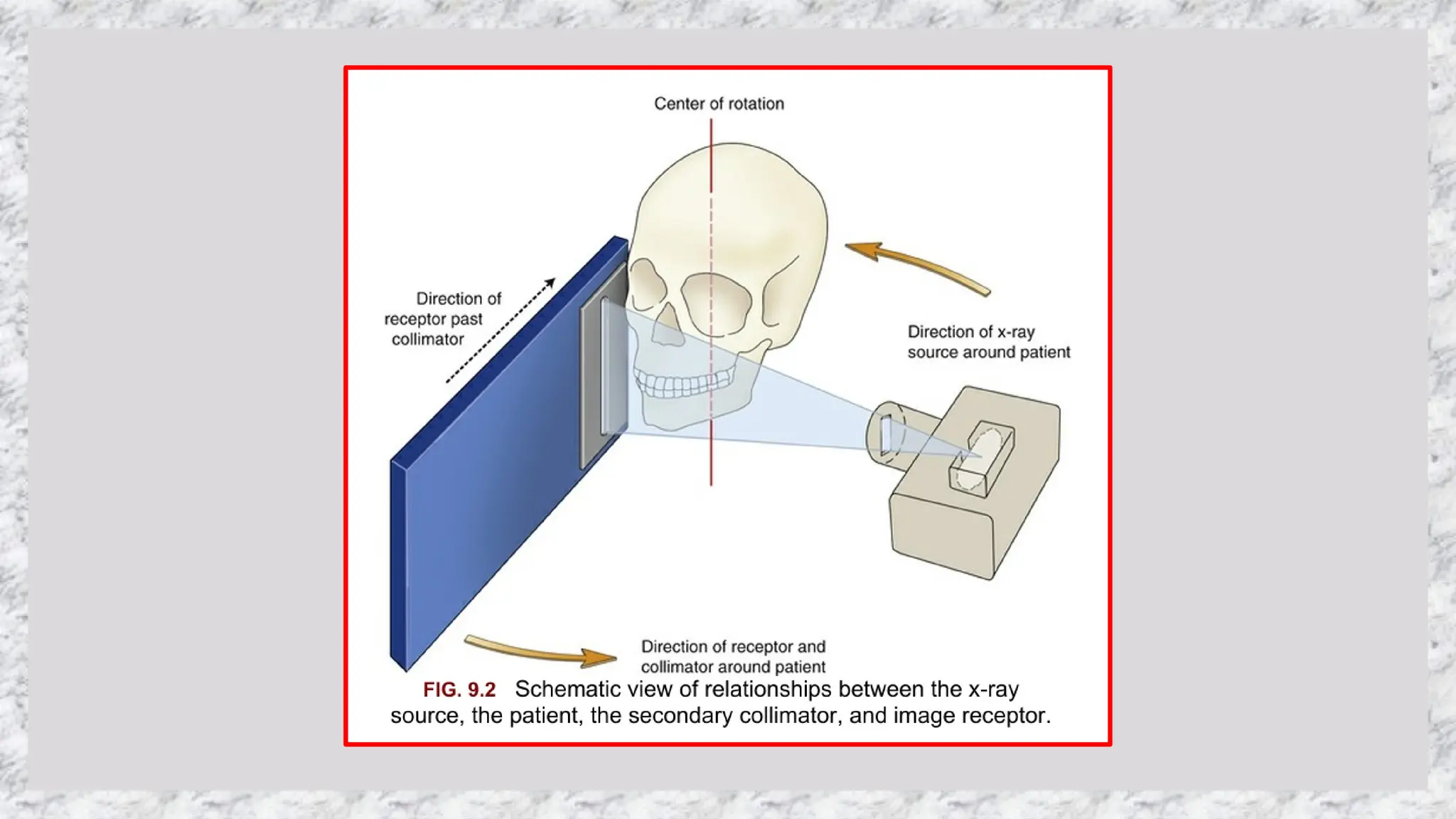
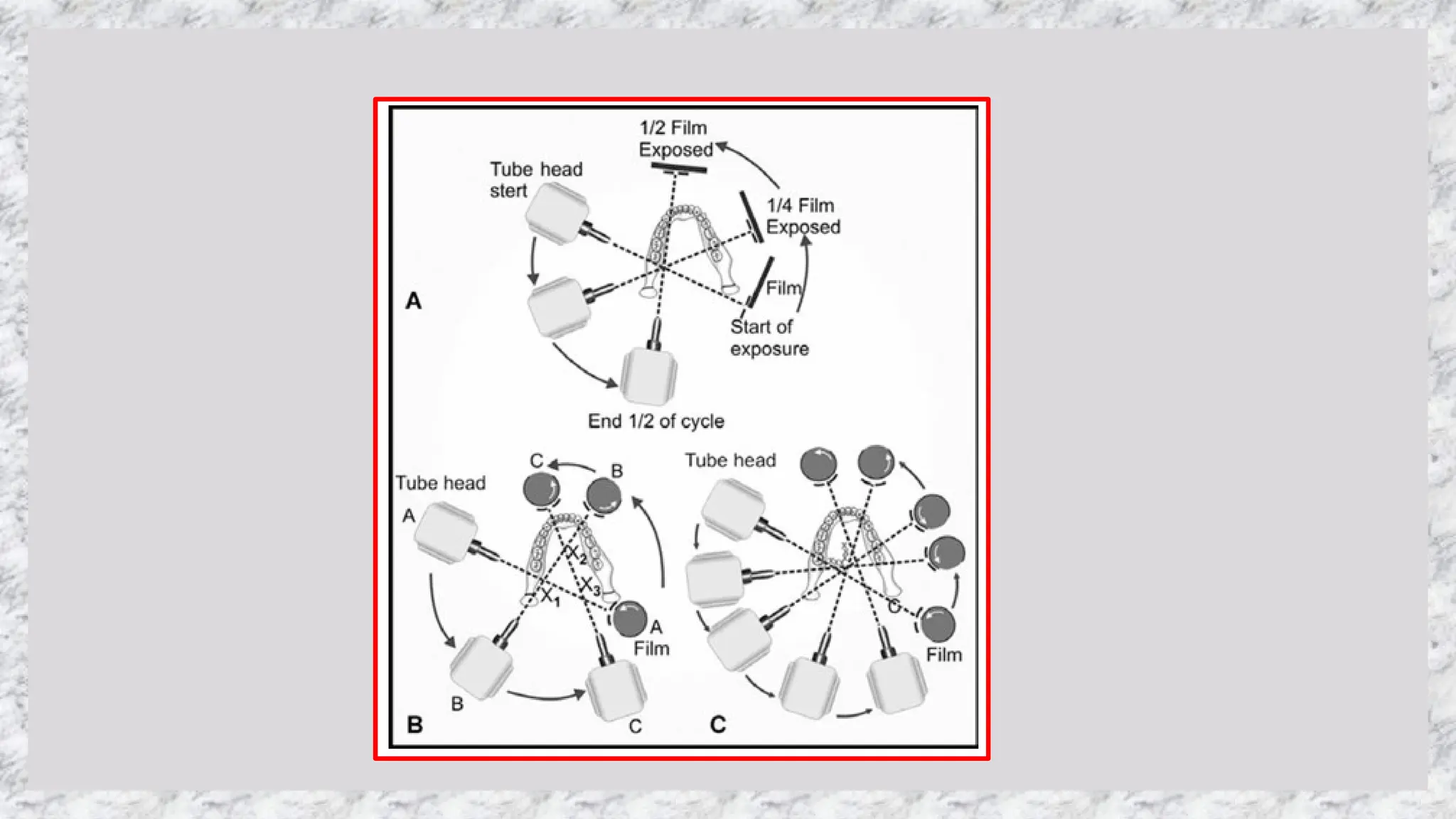
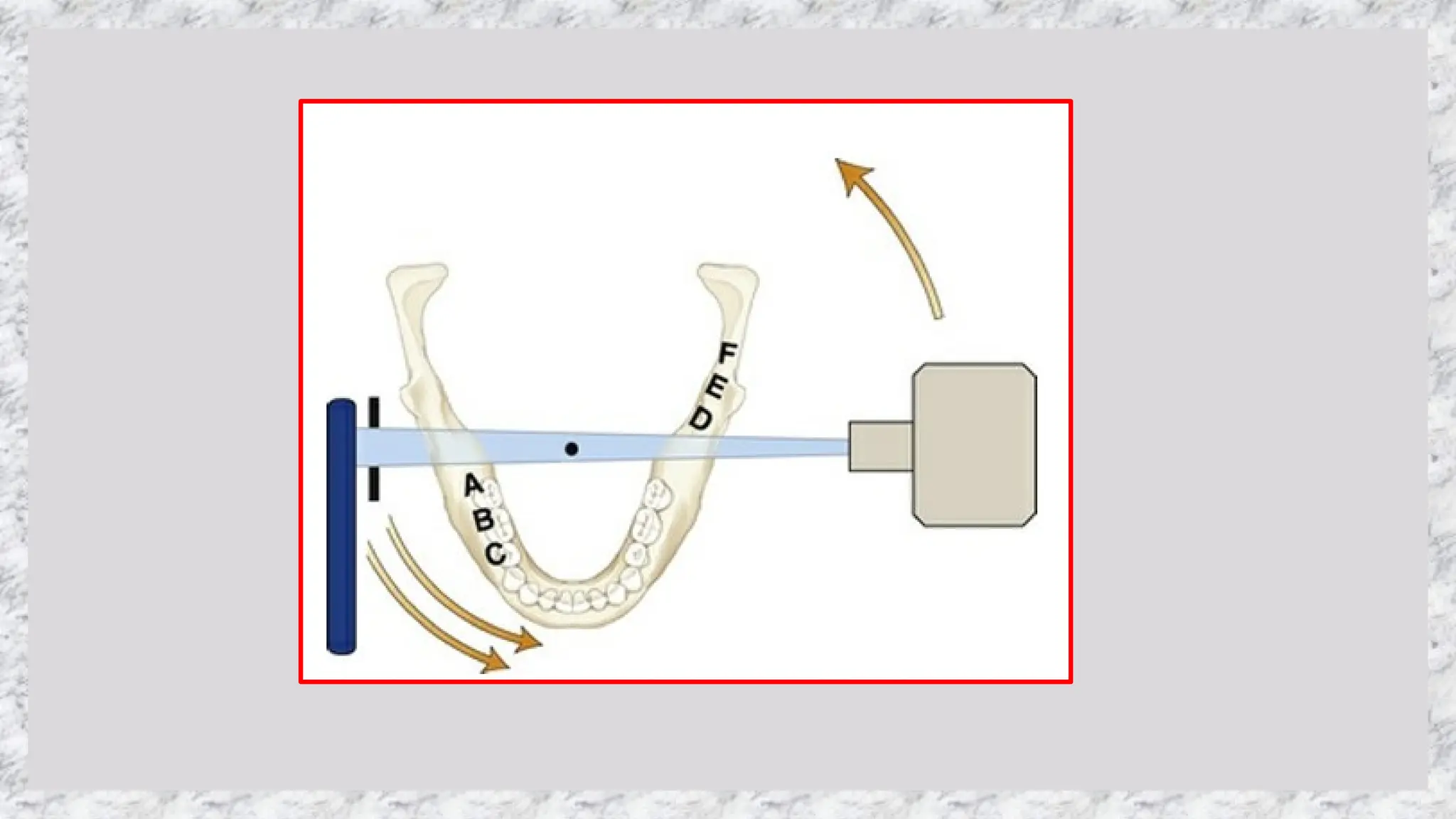
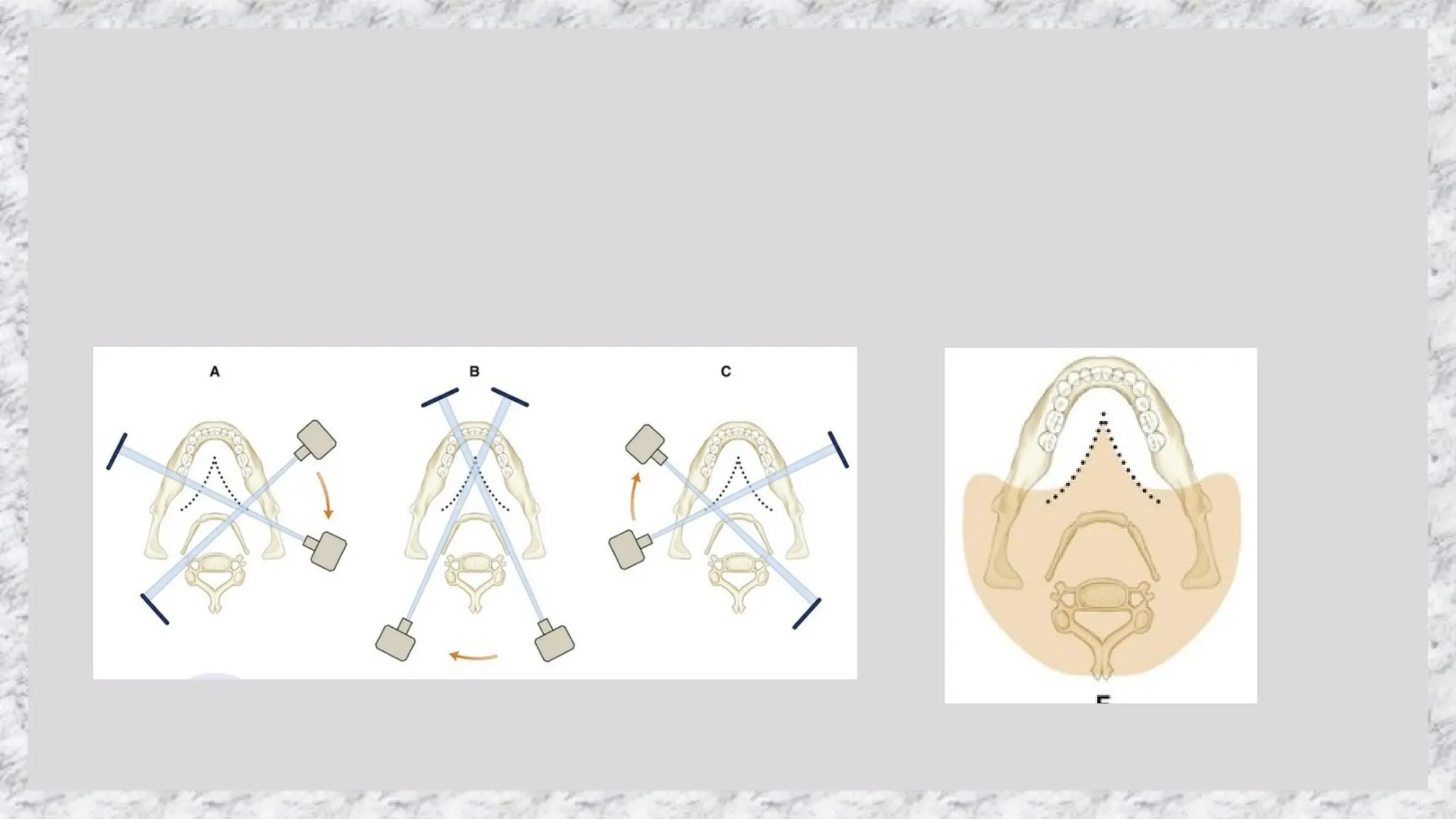

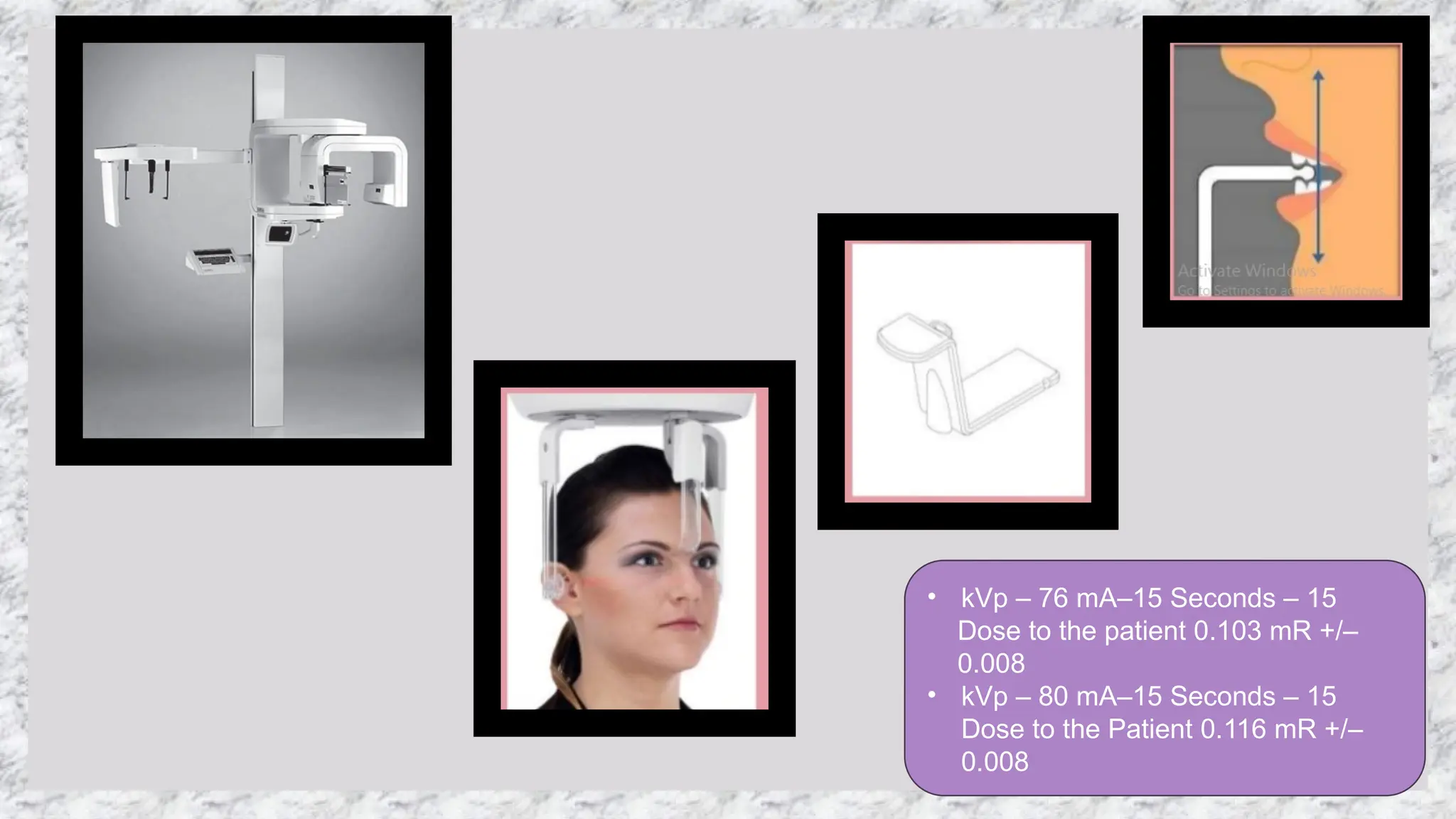
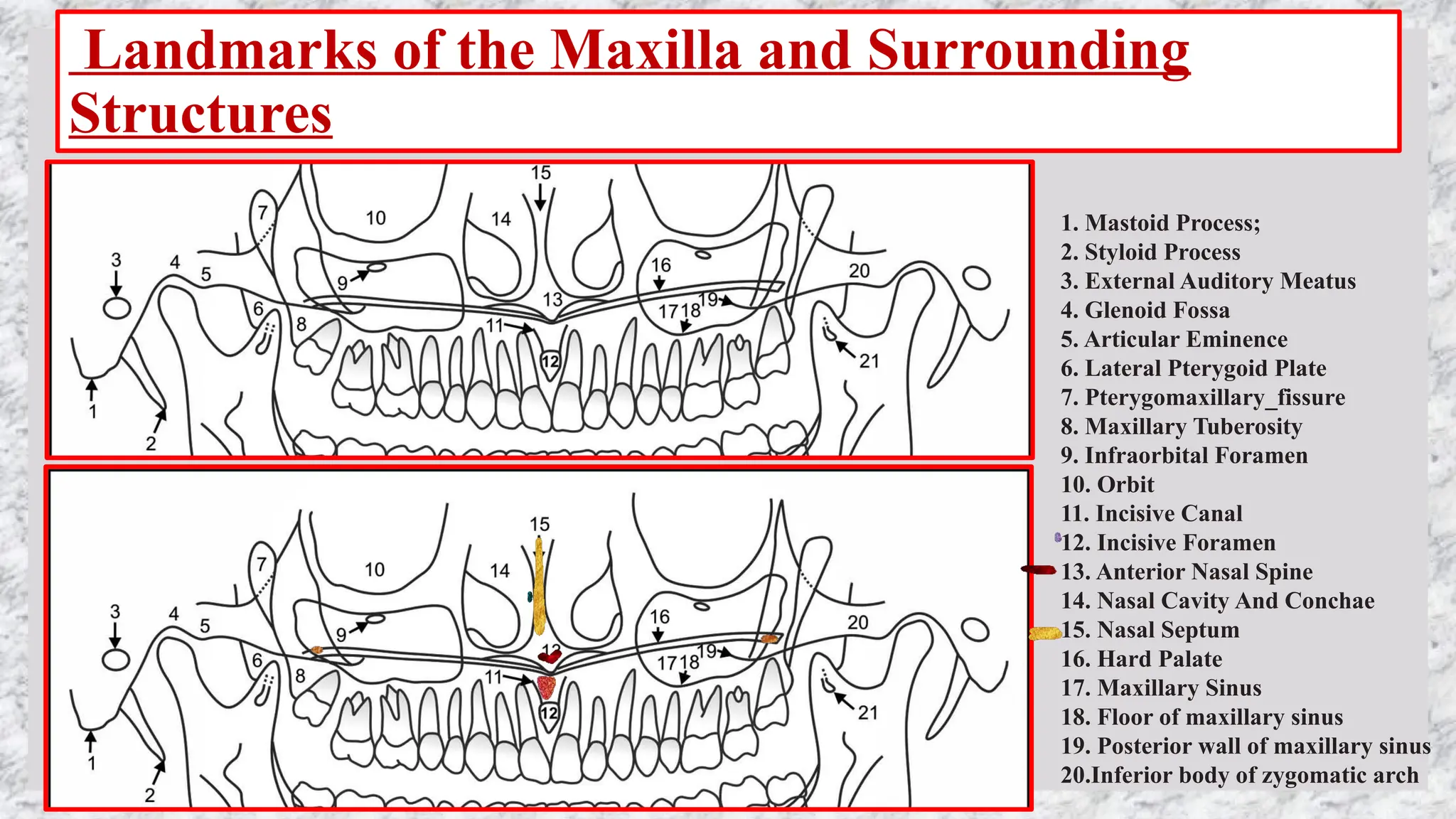
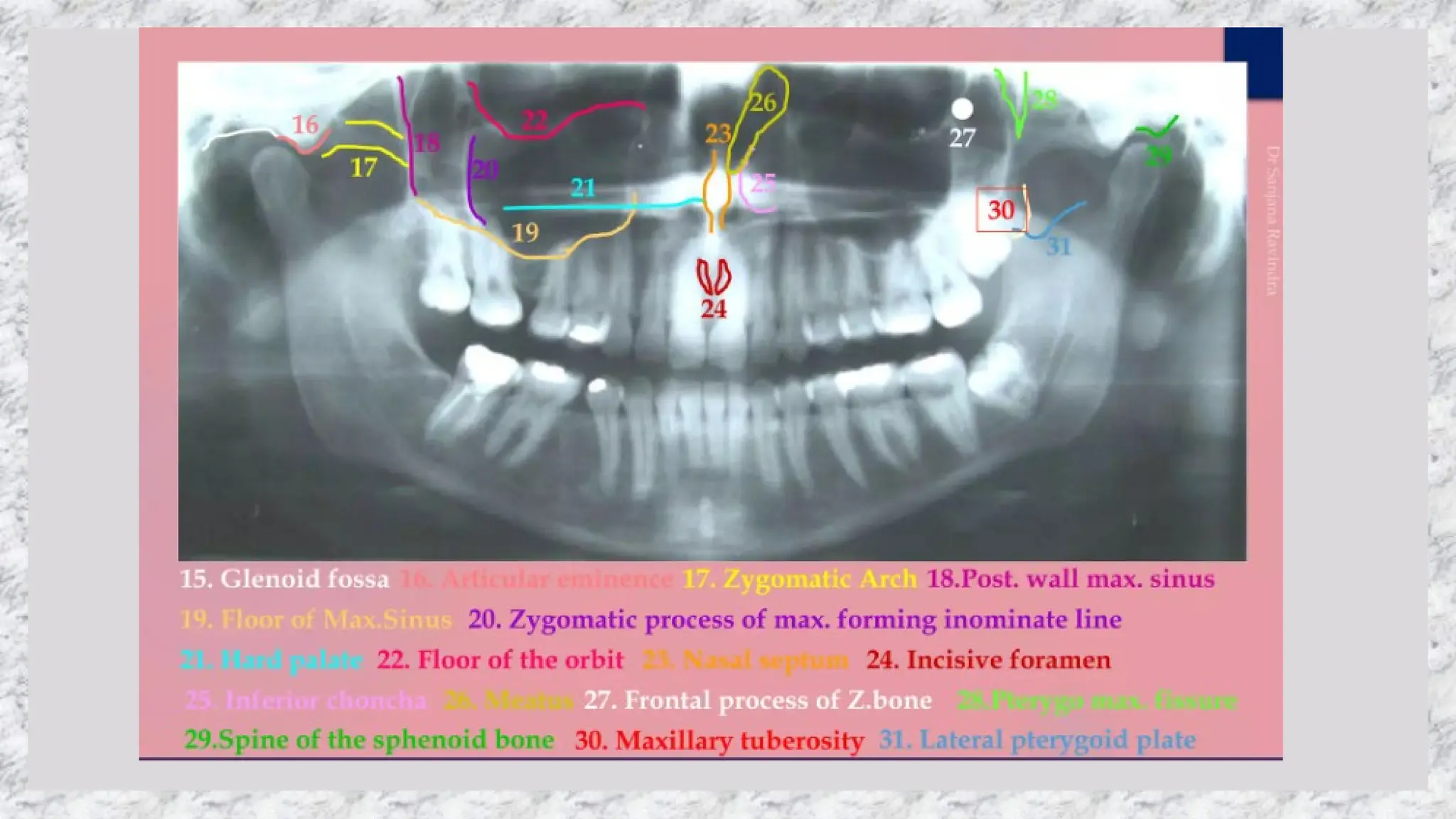
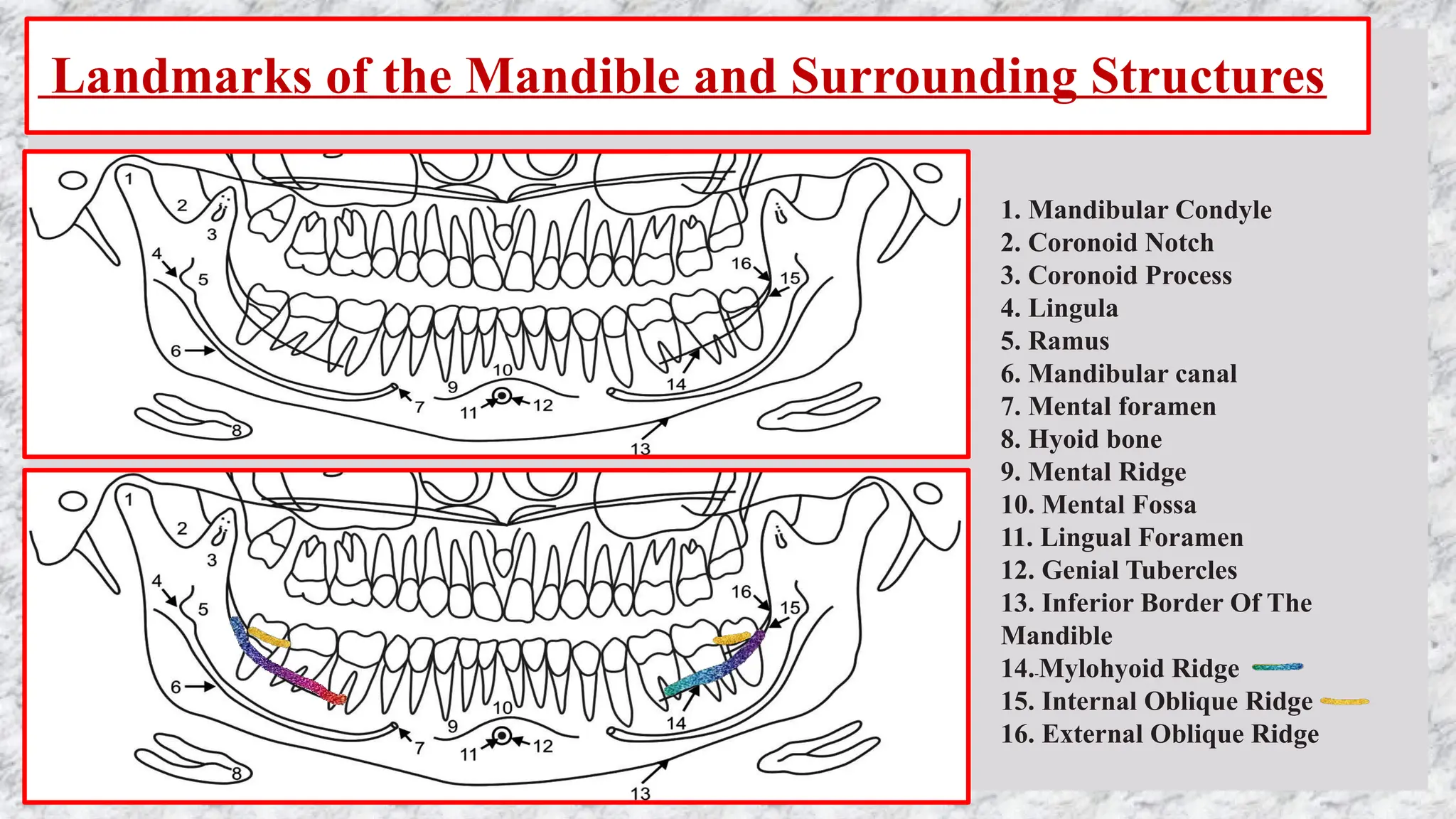
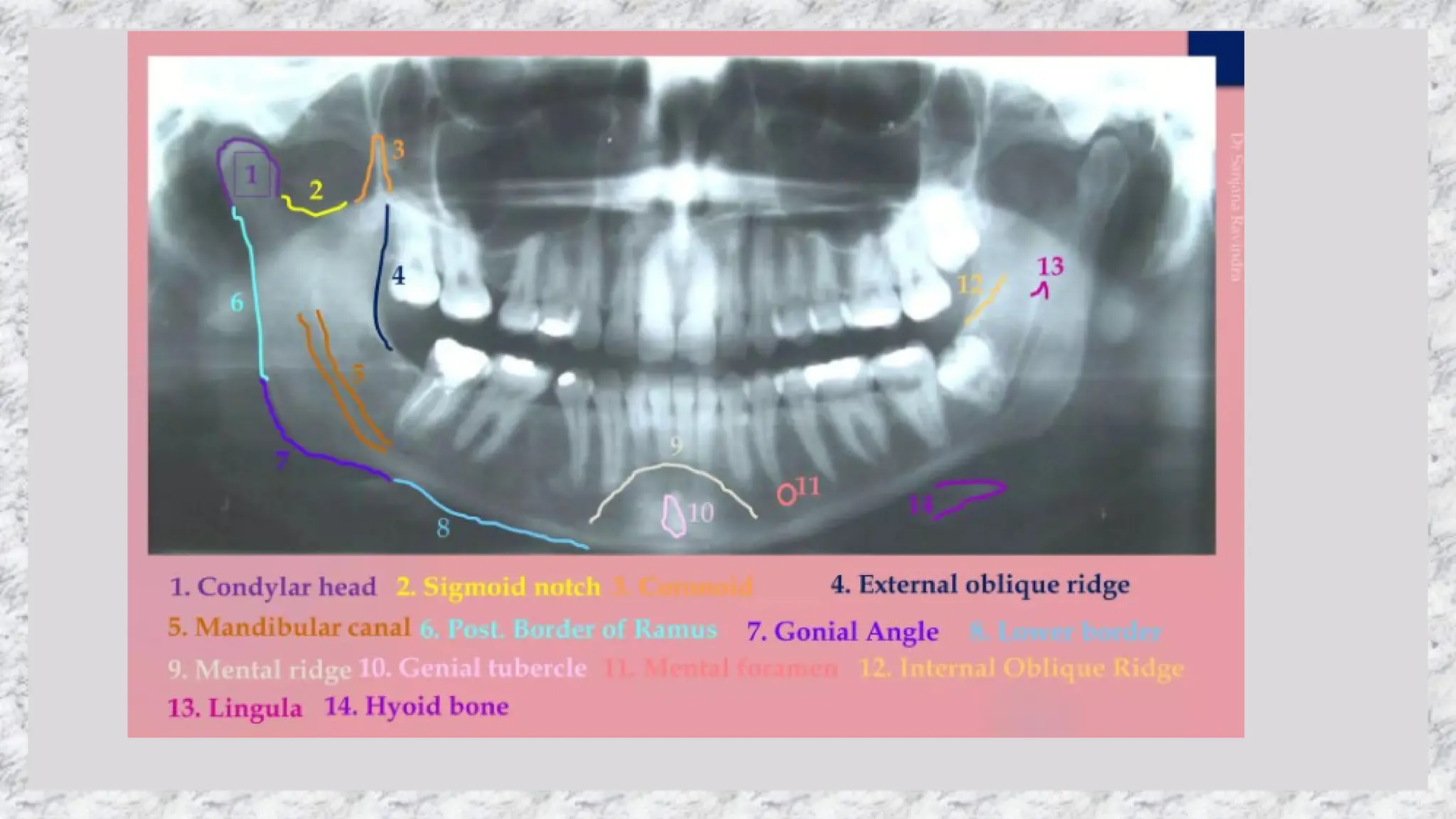


Panoramic radiography is a technique that produces a single image of facial structures, capturing both maxillary and mandibular arches while minimizing interference from overlapping tissues. The procedure utilizes a single rotation of the x-ray source and image receptor, allowing for clear imaging when positioned correctly within a defined focal trough. Key applications include evaluating dental pathology, impacted teeth, and maxillofacial disorders, though it has limitations such as lower resolution and potential image artifacts.























































































