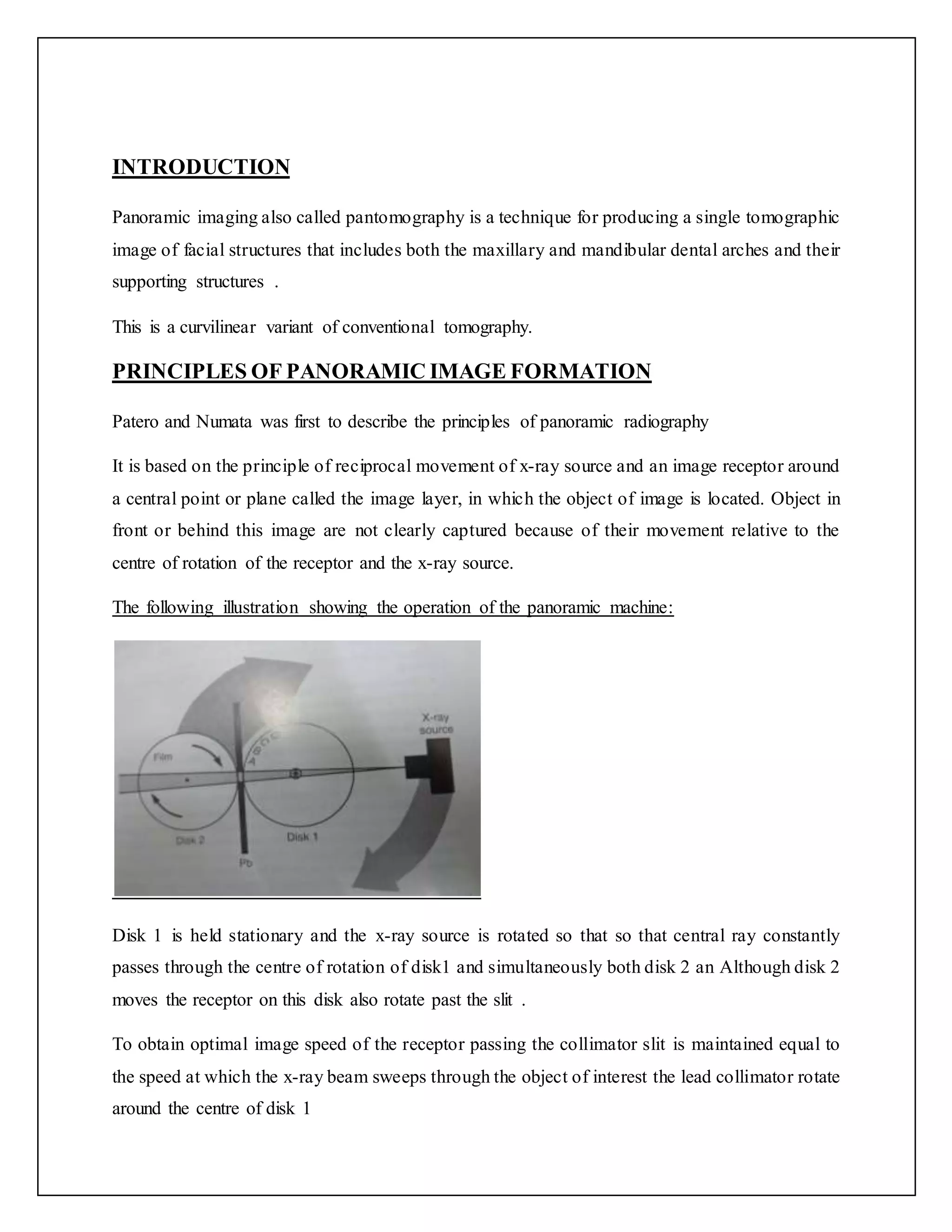
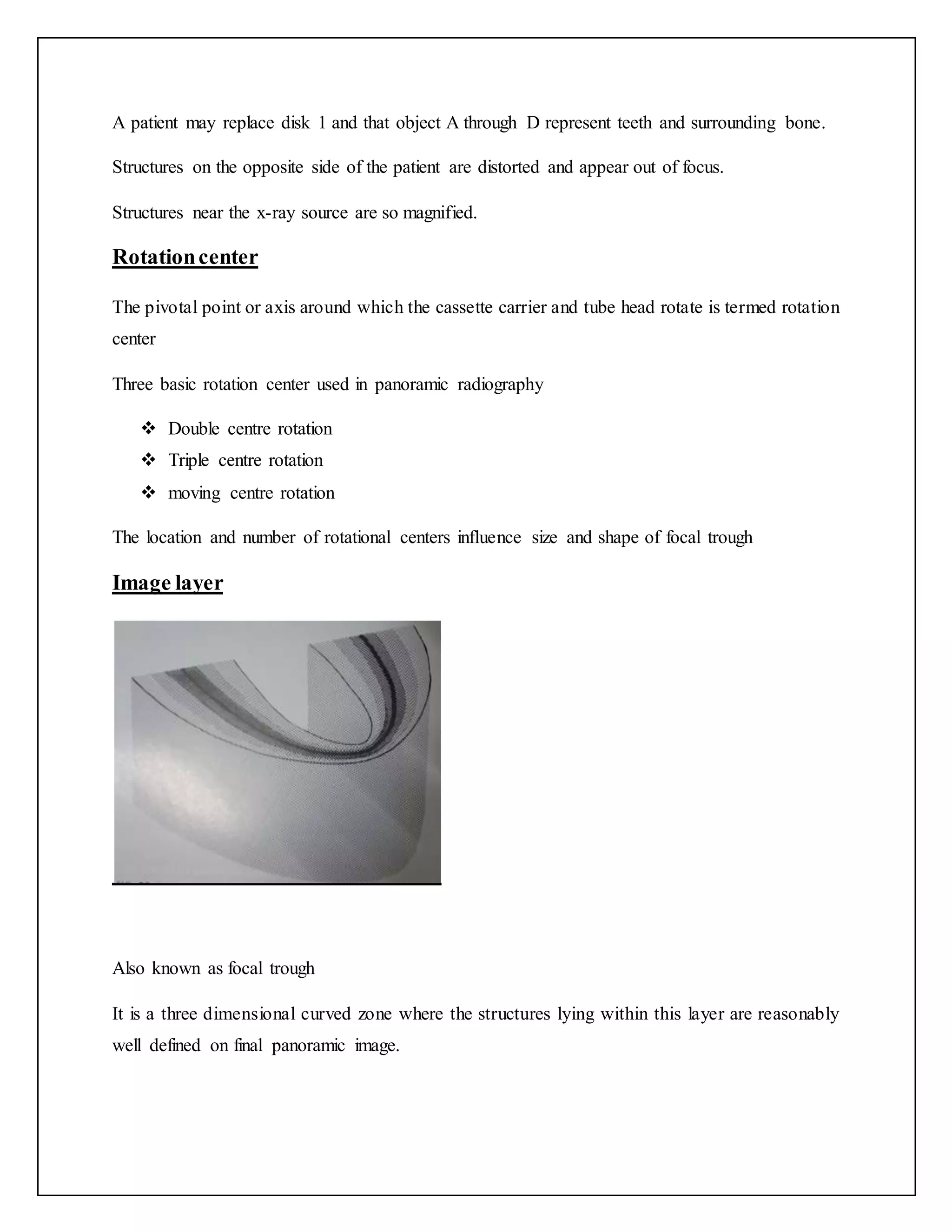
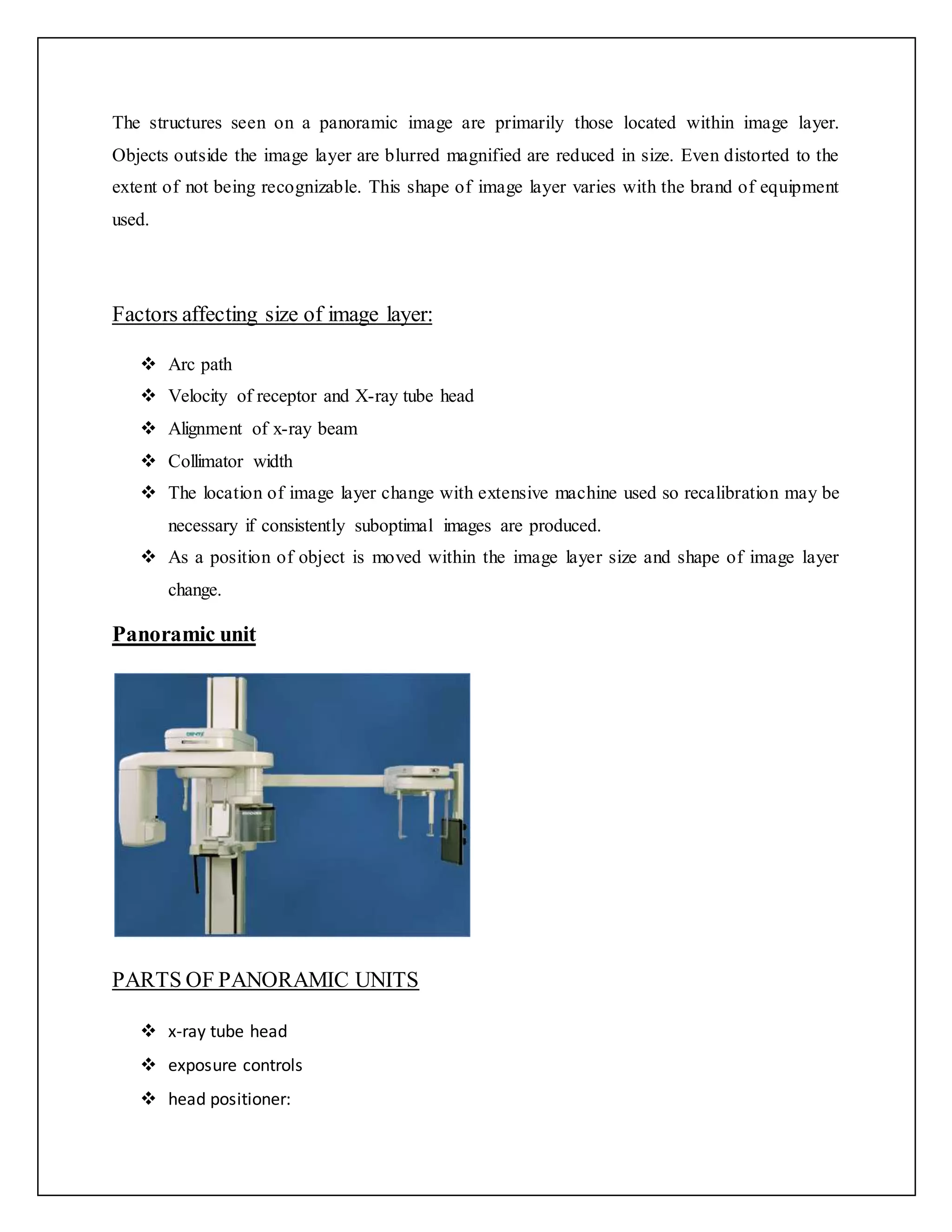
This document provides an overview of orthopantomography (OPG), also known as panoramic imaging. It discusses the principles of panoramic image formation using reciprocal movement of the x-ray source and image receptor around a central rotation point. Key components of panoramic machines and films are described. Proper patient positioning is emphasized to obtain images of the mandible, midfacial region, dentition and soft tissues within the image layer. Advantages include broad coverage with low radiation dose, while disadvantages include potential for distortion and lack of detail. Indications for OPG use include dental trauma, implants, orthodontics and lesion evaluation.