Downloaded 157 times
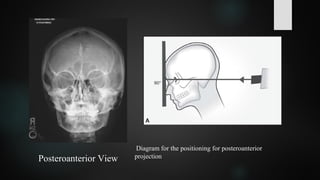
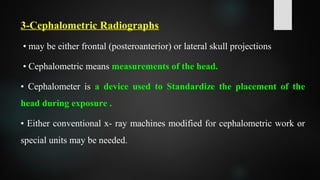





The document discusses various types of extraoral radiographs including lateral jaw projections, posteroanterior views, cephalometric radiographs, Water's views, reverse Towne projections, and submentovertex projections. It describes the purposes, techniques, patient positioning, and anatomical structures visualized for each type of extraoral radiograph. Extraoral radiographs are used to examine large areas of the jaws, skull, sinuses, and temporomandibular joints as well as to detect fractures, lesions, and developmental abnormalities.























































































