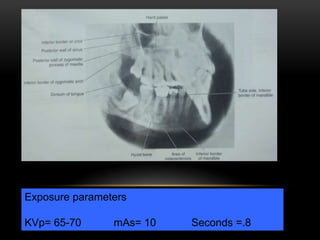
The document discusses various extraoral radiographic techniques, primarily focusing on panoramic imaging and its applications in evaluating maxillofacial structures. It highlights the advantages and limitations of panoramic radiography compared to intraoral films, detailing operational parameters, positioning for different projections, and common errors encountered. The conclusion emphasizes the importance of understanding these techniques for accurate diagnosis while minimizing radiation exposure.































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











