Download to read offline


![case study
Walker A, Boaz A, Hurley
MV. The role of leadership
in implementing and
sustaining an evidence-
based intervention for
osteoarthritis (ESCAPE-
pain) in NHS
physiotherapy services: a
qualitative case study
[published online ahead of
print, 2020 Aug 5]. Disabil
Rehabil. 2020;1-8.
doi:10.1080/09638288.20
20.1803997](https://image.slidesharecdn.com/qualitativeresearchdesign-210205141215/85/Qualitative-research-design-10-320.jpg)
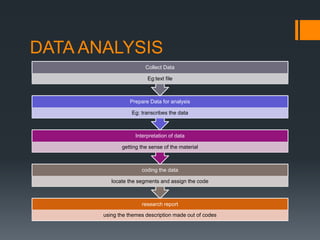
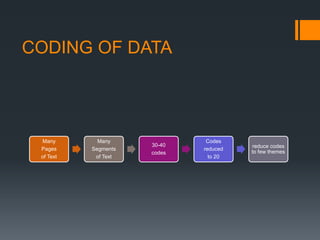
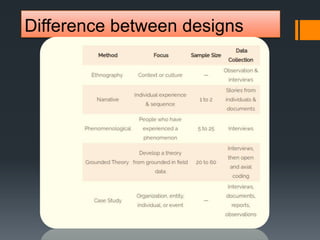
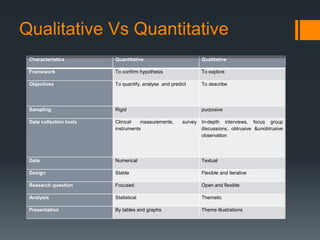

This document outlines the objectives and key aspects of qualitative research design. It discusses qualitative statement, types of qualitative designs including phenomenology, grounded theory, case study, narrative synthesis, ethnography, historical research and action research. It also covers sampling design, observational design, operational design, data analysis design and the differences between qualitative and quantitative designs. Key points covered include that qualitative research aims to understand and describe central experiences or processes for participants through methods like interviews and observations. Different qualitative designs have different focuses such as experiences for phenomenology or groups for ethnography. The document provides examples of studies for each design type.









































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












