The document outlines a workshop on fitting psychosocial assessment into subjective questioning for physiotherapy practice, with an emphasis on integrating biopsychosocial factors. It discusses the importance of developing psychosocial questioning skills to better manage patients' pain, guide self-management, and address barriers to service. The aims include improving knowledge among physiotherapy cohorts about the role of physioline consultations and strategies for identifying when to self-manage or refer patients appropriately.

![References
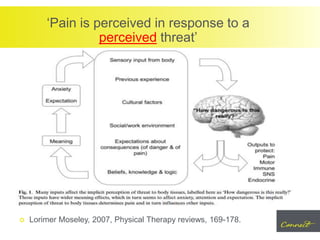
Lorimer Moseley, 2007, Physical Therapy reviews, 169-178
Plisky et al (2006), Star excursion balance testing as a predictor
of lower limb extremity injuries in high school basketball players,
Journal of orthopaedic sports medicine, 36 (12).
Brooks JC, Nurmikko TJ, Bimson WE, Singh KD, Roberts N.
fMRI of thermal pain: effects of stimulus laterality and
attention. Neuroimage. 2002;15:293–301. [PubMed]
http;//www.bodyinmind.org](https://image.slidesharecdn.com/communityservicesphysioline-d-180127215207/85/Psychosocial-Management-Subjective-Assessment-27-320.jpg)









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)