Pupillary pathway and its abnormality.
•Download as PPTX, PDF•
13 likes•1,235 views

This document discusses the pupillary pathway and various pupillary disorders. It begins by describing the development of the pupil from the pupillary membrane. It then discusses the muscles that control pupil size and various reflexes like the light and accommodation reflex. It describes different types of pupil abnormalities including iris colobomas, aniridia, traumatic causes and neurological causes. Specific disorders like Horner's syndrome and Adie's tonic pupil are explained in detail. Pharmacological tests to localize lesions in different parts of the pupillary pathway are provided. The document concludes by mentioning some references.

More Related Content
What's hot
What's hot (20)
Similar to Pupillary pathway and its abnormality.
Similar to Pupillary pathway and its abnormality. (20)
More from Shreeji Shrestha
Recently uploaded
Recently uploaded (20)
Pupillary pathway and its abnormality.
- 2. Development •pupillary membrane is formed by the condensation of 2nd wave mesodermal tissue surrounding the margin of the optic cup and tunica vasculosa lentis. • The peripheral part of the pupillary membrane gets vascularised. •The central part is eventually completely absorbed forming the pupil. •Pupil is formed by the complete absorption of the central part of pupillary membrane
- 3. • Pupillary membrane begins to degenerate at to degenerate at 8th month • Iris stroma and dilator muscle is I'm is immature hence pupil remain co nstri constricted at birth
- 4. Persistent pupillary membrane Polycoria Iris coloboma- associated with CHARGE syndrome, turner , klinefelter Aniridia
- 5. Acquired causes of pupil irregularity • Blunt trauma - focal tear in sphincter muscle • Iridodialysis - outer edge of iris is torn from ciliary attachment • Synechiae - IO inflammation can damage iris leading adherence to lens or cornea • Neovascularization- distort iris and impair reactivity • Surgical procedure in anterior segment, cataract • Tadpole pupil- focal spasm of iris dilator muscle • Midbrain corectopia- rostral midbrain disease
- 6. PUPIL ● Round in shape and relatively equal in size ● Located inferonasally to the centre of cornea ● Normal pupil range from 3 to 4mm in ambient light conditions ◦ Miotic pupil- less than 2mm ◦ Mydriatic pupil- greater than 7mm
- 7. PUPIL SIZE ● Determined by ◦ Level of retinal illumination ◦ Level of arousal ◦ Amount of ambient light ◦ Age ◦ Small pupil: Sleep, infants, old age ◦ Large pupil: Excitement, arousal,seizures, increased IOP
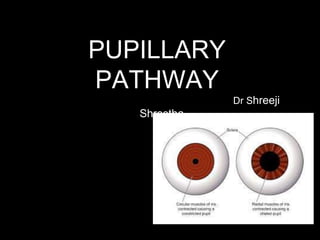
- 9. Pupil Contraction and Dilation ● Controlled by two muscles of iris ◦ Sphincter muscle (pupil constriction) ●Innervated by the parasympathetic nerve ◦ Dilator muscle (pupil dilation) ●Innervated by the sympathetic nerve
- 10. FUNCTIONS OF PUPIL •Pupil movement in response to changing light intensity helps in optimizing retinal illumination to maximize the visual perception •Improves the image quality of the retina when the steady state pupil diameter is small. •Small pupil increases the depth of focus of the eye’s optical system similar to pinhole effect of camera by limiting rays entering cornea
- 13. Pupillary reflex ● Light reflex ● Near reflex ● Psychosensory reflex
- 14. Llight reflex Preganglionic parasympathetic fibers Postganglionic parasympathetic fibers Contraction of sphincter muscle
- 15. Clinical aspect Left Right Damage to left optic nerve/pretectal nucleus light in LE- no direct plus consensual light reflex in right eye Light in right eye- direct + consensual light reflex present Damage to left EWN/ occulomotor nerve/ ciliary ganglion Light in LE light in RE LE- no change LE - no change RE- pupil constrict. RE- constrict
- 16. Accommodation reflex • Def- ability of eye to see near object when focusing on far object • Stimulus- sudden exposure of eye to near object • Response- constriction of pupil Convergence of eyeball Increase curvature of lens
- 17. Near reflexshort ciliary nerve Contraction of ciliary muscle- increase in curvature Contraction of constrictor pupillae- constrict pupilContraction of MR- convergence of eyeball
- 18. Dilatation has 2 causes: •Simply abolition of light reflex with consequent relaxation of the sphincter pupillae •Contraction of dilator pupillae supplied by sympathetic nervous system Darkness reflex
- 19. Psychosensory reflex •Dilatation of pupil in response to sensory and psychic stimuli •Mechanism of psychosensory reflexes is a cortical one and apparently the pupil dilatation in these results from 2 components- ✓Sympathetic discharge to the dilator pupillae ✓Inhibition of parasympathetic discharge to the sphincter pupillae.
- 20. Abnormal Pupillary Reactions ● Afferent pupillary defect • Total afferent pathway defect (TAPD) or Amaurotic pupil • Relative afferent pathway defect (RAPD) or Marcus Gunn pupil • Wernicke’s hemianopic pupil ● Efferent pupillary defect • Tonic pupil • oculomotor nerve palsy • Pharmacologic mydriasis ● Light near dissociation • Argyll Robertson pupil
- 21. TAPD/amaurotic pupil • Caused - complete optic nerve or retinal lesion Total blindness on affected side • Ctd by: direct light reflex on affected side - abs consensual light reflex on normal side- abs When the normal eye is stimulated, both pupils react normally near reflex - normal Diffuse illumination - both pupil are equal
- 22. Relative afferent pathway defect / Marcus gunn pupil Paradoxical response of pupil to light -relative measurement of input of one eye compared to other eye Cause - incomplete nerve lesion or. a severe retinal disease Central serous retinopathy or cystoid macular edema Central or branch retinal vein/artery occlusion Retinal detachment Anterior ischemic optic neuropathy Optic neuritis Compressive optic neuropathy Intraocular hemorrhage-AC or vitreous
- 23. RAPD grading Grade 1+: A weak initial pupillary constriction followed by greater redilatation Grade 2+: An initial pupillary stall followed by greater redilatation Grade 3+: An immediate pupillary dilatation Grade 4+: No reaction to light
- 24. Measurement of RAPD Neutral density filters ● Estimation of the amount of RAPD is in log units using NDF placed infront of better eye and provides idea of how much visual field damage is present. ● NDF balances asymmetry of pupil btn 2 eyes ● Loss of central 5º of visual field results in RAPD of 0.3 log units. ● Loss of entire central field 10º causes RAPD of 0.6-0.9 log units.
- 26. • Tilting test: If very small asymmetry is suspected (eg hippus) confirm by tilting the RAPD to right and left using 0.3 log unit filters. • Infrared videography: helps to examine both pupil clearly in dark and to establish dilatation lag of horner’s pupil. • Computerized pupillometry: helps to record dynamics of pupil movement and analyzed by software • Pupil perimetry: Video camera is pointed at pupil and amplitude of each light reaction is measured
- 27. Wernicke hemianopia pupil • Cause- optic tract lesion • Light reflex- ipsilateral direct & contralateral consensual absent when light shown in termporal half of affected retina & nasal half of opposite side
- 28. Efferent pupillary defect ● Interferes with contraction or dilatation of pupil due to the damage in midbrain, peripheral nerves that supply iris muscles, or in the iris muscles itself causing anisocoria ● Damage to parasympathetic or sympathetic nerves that supply iris
- 29. Anisocoria equal in both dim & bright light: - Physiologic/primary Anisocoria: 20% of the individuals Difference in pupil diameter<1.0mm Anisocoria greater in dim light( if iris dilated is paretic or sympathetic palsy) ● Mechanical anisocoria: Previous trauma/ surgery Inflammation ● Pharmacological anisocoria: Unilateral use of medications like pilocarpine ● Horner syndrome
- 30. Physiologic anisocoria ● Dim light- right pupil is slightly larger than left ● Bright light both pupil constricts ● After instillation of cocaine both pupil dilates
- 32. Horner syndrome ● Lesion at any point along oculosymphathetic pathway • Characterized by : 1) ptosis - paralysis of muller muscle 2) miosis - paralysis of dilator pupillae 3) anhidrosis - reduced sweating on face and neck when lesion is below SCG 4) apparent enophthalmos 5) Dilation lag : when lights are turned off the horner’s pupil dilates more slowly than normal pupil does 6) Heterochromia irides: when sympathetic innervation is interrupted early in life 7) light reflex and Near reflex - normal ● Anisocoria is more apparent in dim illumination.
- 33. Causes of Horner syndrome
- 34. Pharmacological Tests for horner syndrome ● Cocaine 4 or 10%: instilled in both eyes Cocaine blocks reuptake of noradrenaline so causes pupillary dilatation In Horner syndrome no NA is secreted in first place so no effect seen Result: Normal pupil dilate but Horner pupil does not dilate. ● Apraclonidine 0.5% or 1.0% Alpha-1 agonist In sympathetic denervated eyes, dilator muscle develops adrenergic supersensitivity causing pupillary dilatation Result: Horner pupil dilates but normal pupil is unaffected
- 35. • Hydroxyamphetamine test - localize site of lesion A. Postganglionic - pupil will not dilate at all B. Preganglionic / central lesion - pupil will dilate normally • Decentralization supersensitivity - Horner pupil dilate more than normal - preganglionic
- 36. Central Preganglionic Postganglionic Hypothalamic signs: disturbed sleep, temperature Lungs and breast malignancy has spread to thoracic outlet Ipsilateral vascular headache Brainstem- vertigo, sensory deficit history of injury / surgery in neck, chest tumor in cavernous sinus associated III, IV, VI palsy Meningeal signs Anhydrosis, brachial plexus palsy, vocal cord palsy ICA dissection: face/neck pain neck bruit Retinal artery occlusion
- 37. Tonic pupil ● Traumatic iridoplegia (sphincter rupture, pigment dispersion, angle recession) ● Angle-closure glaucoma (ischemia of the iris sphincter) ● Fixed pupil after anterior segment surgery ● Bound down iris (synechia) after iritis ● Pharmacologic pupil- mydriatic medications ● Adie tonic pupil ● Third nerve palsy Anisocoria Greater in Bright Light(iris sphincter is par
- 38. Adie’s tonic pupil •Caused by denervation of the post ganglionic supply of the sphincter pupillae and ciliary muscle •which may follow viral illnessUsually unilateral •Typically affects healthy young women (U/L) •Affected pupil is large and irregular •Light reflex is absent •Near reflex is slow and tonic •Accomodative paresis •May be associated with mild regional impairment of corneal sensations •May be associated with absent knee jerk
- 39. Third nerve palsy ● Pupillary dysfunction associated with ptosis and limitation of extraocular mobility ● pupil mid-dilated Maximum anisocoria occurs in bright light ● Aneurysms at the junction of internal carotid and posterior communicating artery must be excluded ● 0.125% pilocarpine no constriction but constrict with 1%
- 41. Light near dissociation Condition where light reflex is absent or sluggish but near response is normal
- 42. Argyll Robertson pupil •Caused by the lesion in the region of tectum •Usually bilateral but asymmetrical •Pupils small in size and irregular •Light reflex is absent but near reflex is present •Pupils dilate very poorly with mydriatics
- 43. Pharmacology Miotics •Parasympathomimetics (sphincter stimulators): i. Direct acting: pilocarpine ii. Indirect acting or cholinesterase inhibitors: physostigmine •Sympatholytics 1. Alpha adrenergic blocker: phenoxybenzamine and tolazoline •Others miotics: histamine, morphine Mydriatics •Sympathomimetics: adrenaline, phenylephrine, hydroxyamphetamine, cocaine •Parasympatholytic: atropine, homatropine, tropicamide, cyclopentolate.
- 44. Ciliospinal reflex • B/l pupillary dilatation on nociceptive stimulation on skin of neck • Mediated by 2nd and 3rd order sympathetic nerve
- 45. Other Pupillary Disorders ● Benign Episodic Pupillary Mydriasis- Young, healthy individuals with headache, episodic mydriasis lasting from minutes to hours, mild blurring of vision & periocular discomfort ● Paradoxical Pupillary Reactions- congenital stationary night blindness, congenital achromatopsia. or dominant optic atrophy
- 48. References • Alders physiology • American academy of ophthalmology- neuroophthalmology • Wolf's anatomy of eye • Anatomy and physiology of eye- A K khurana