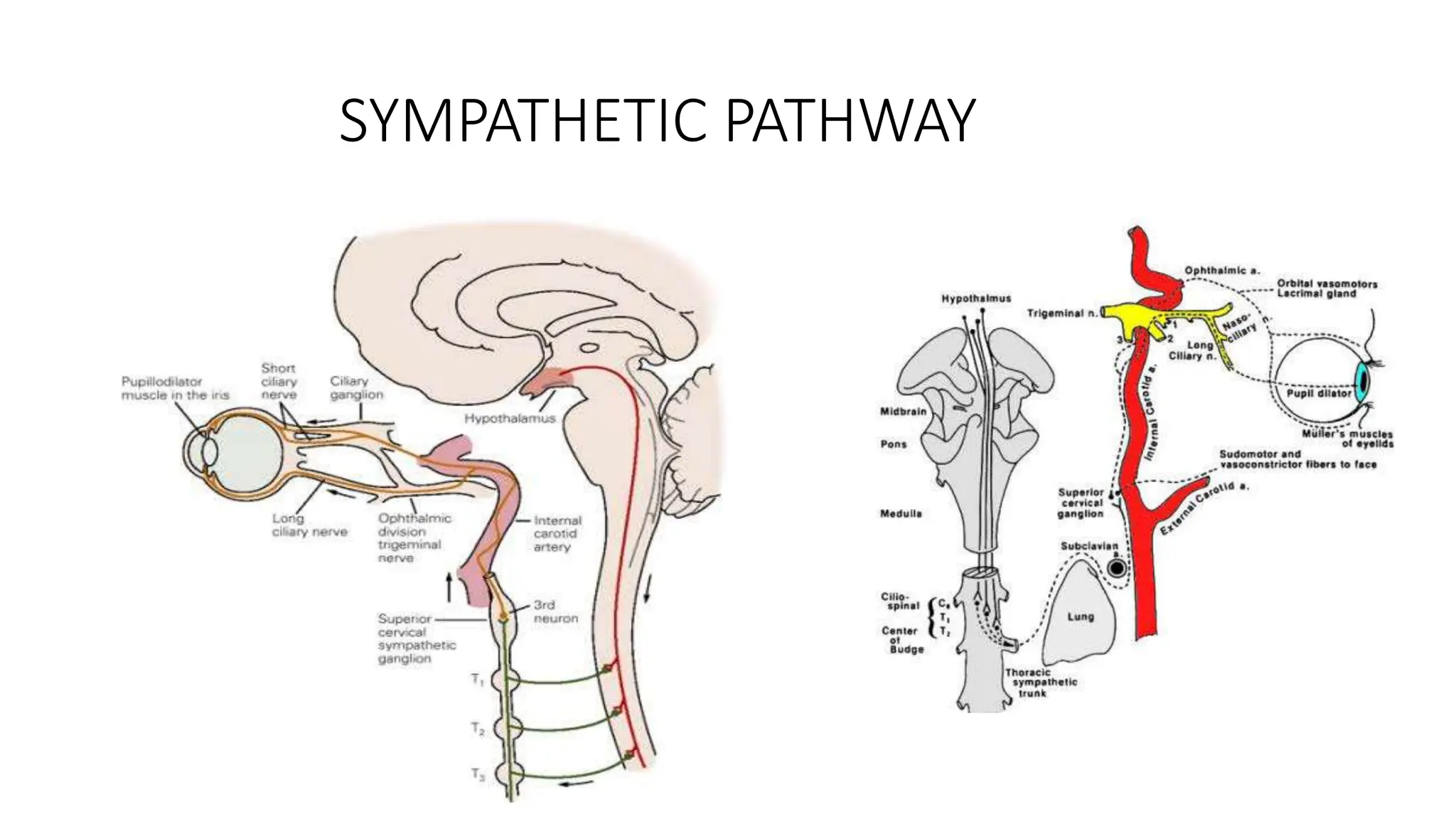
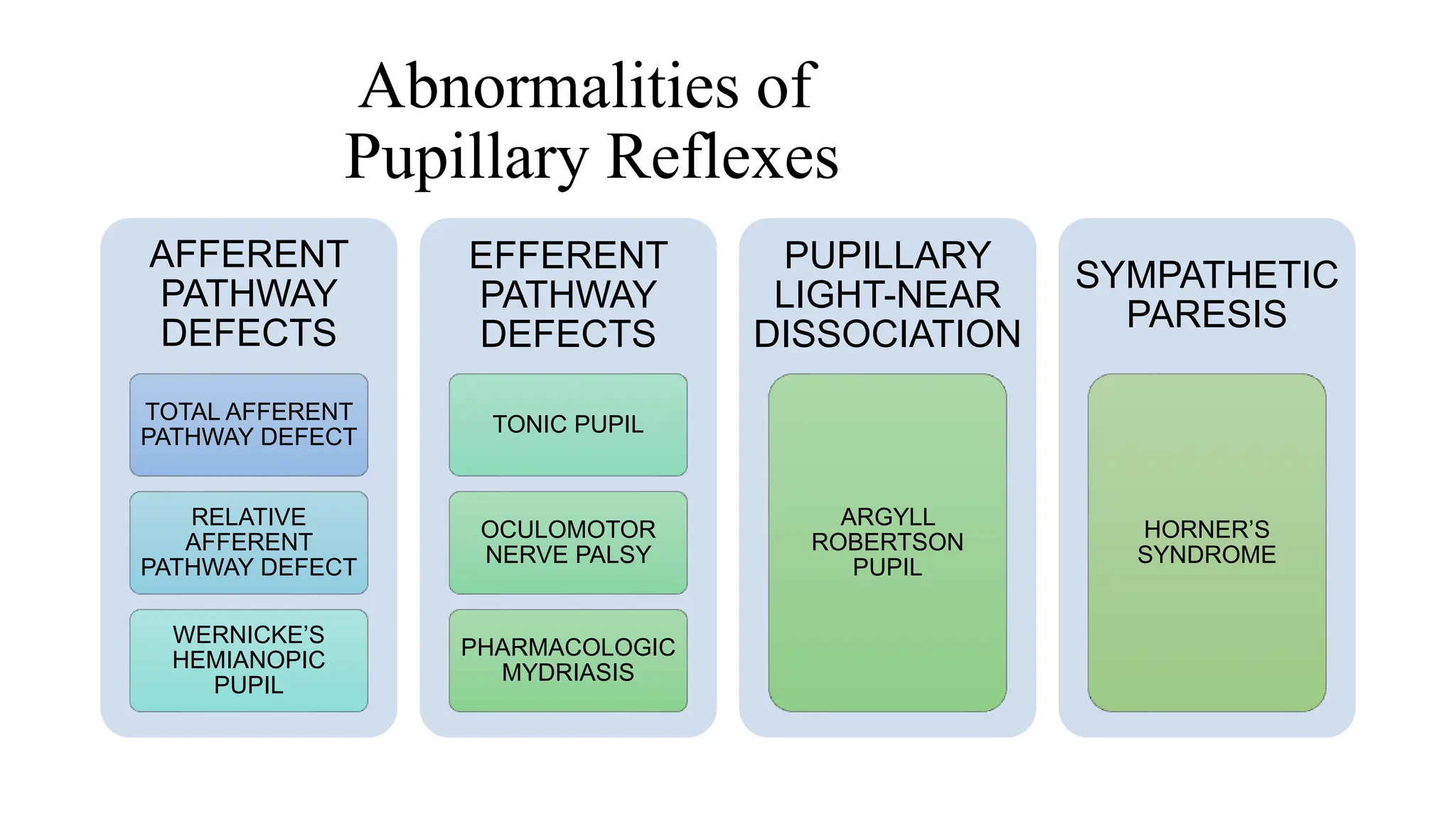
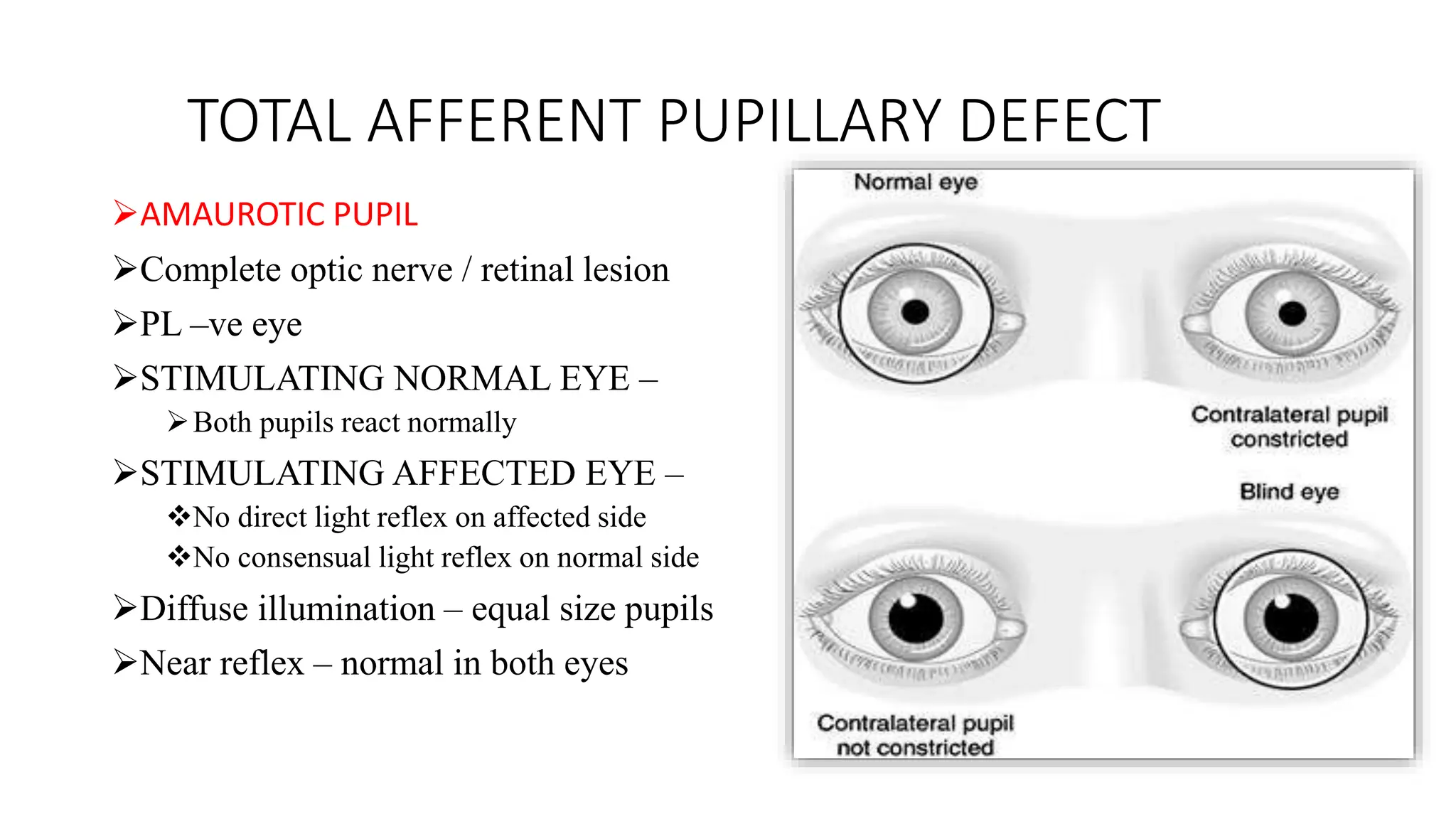
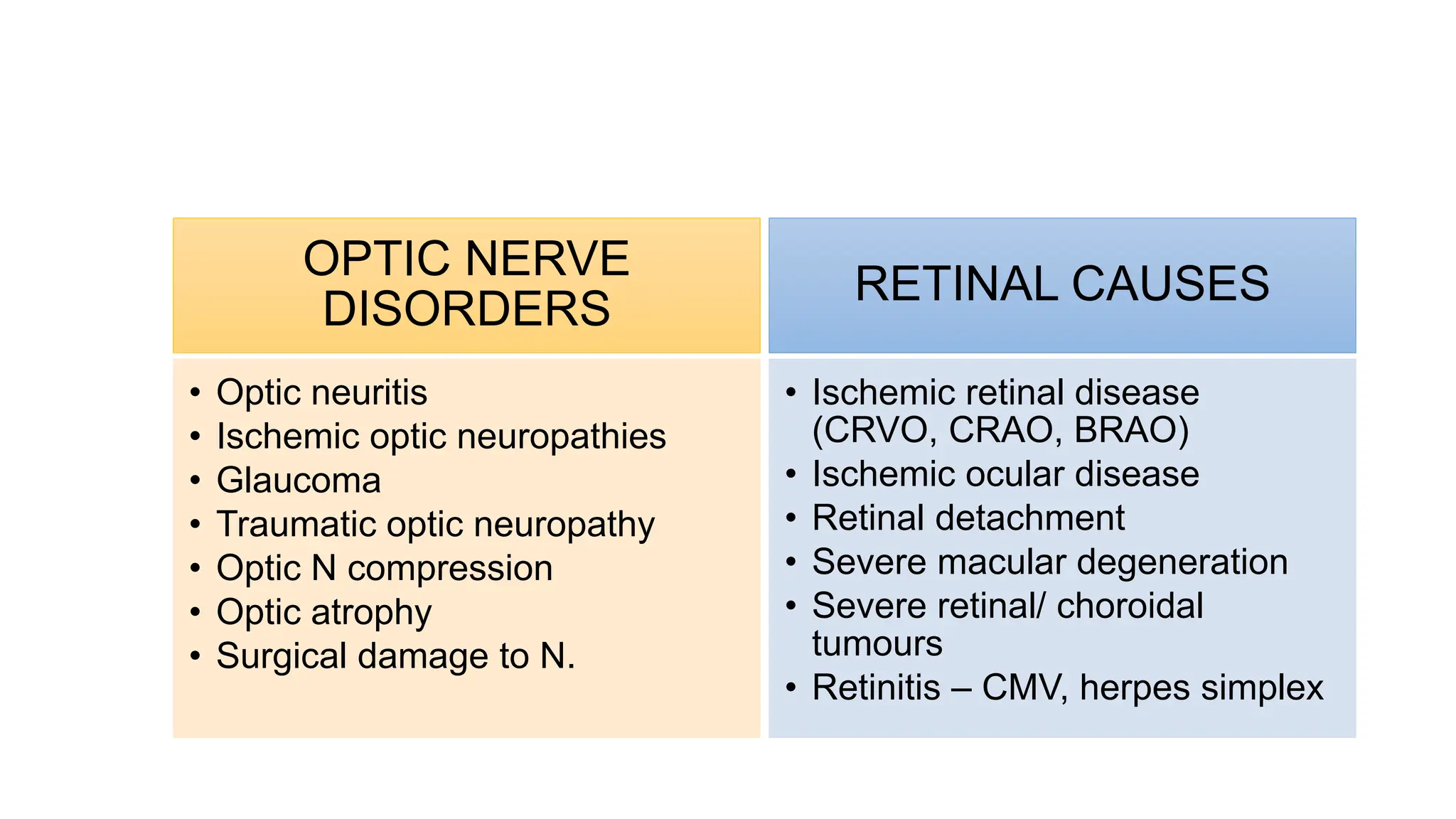
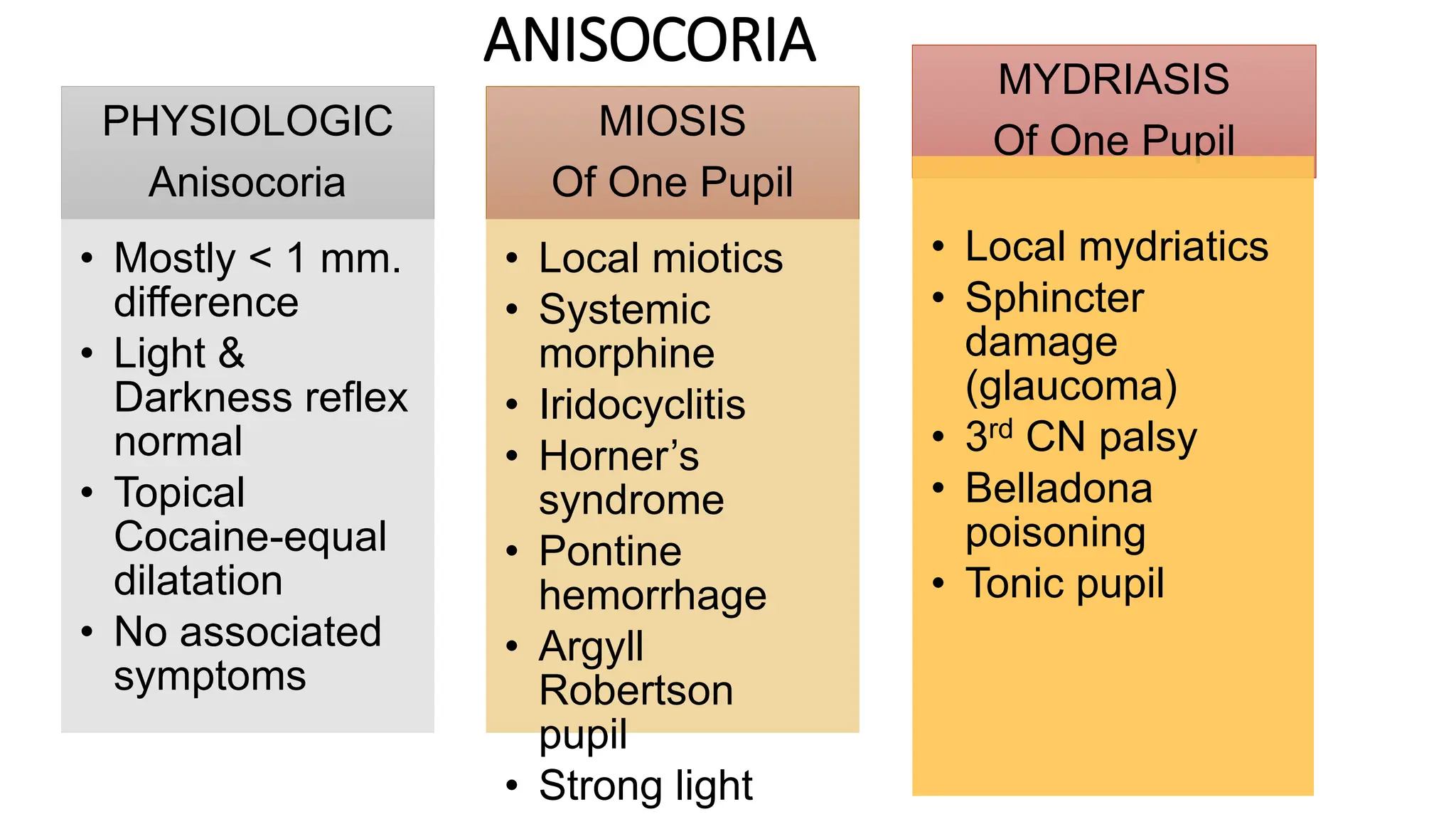
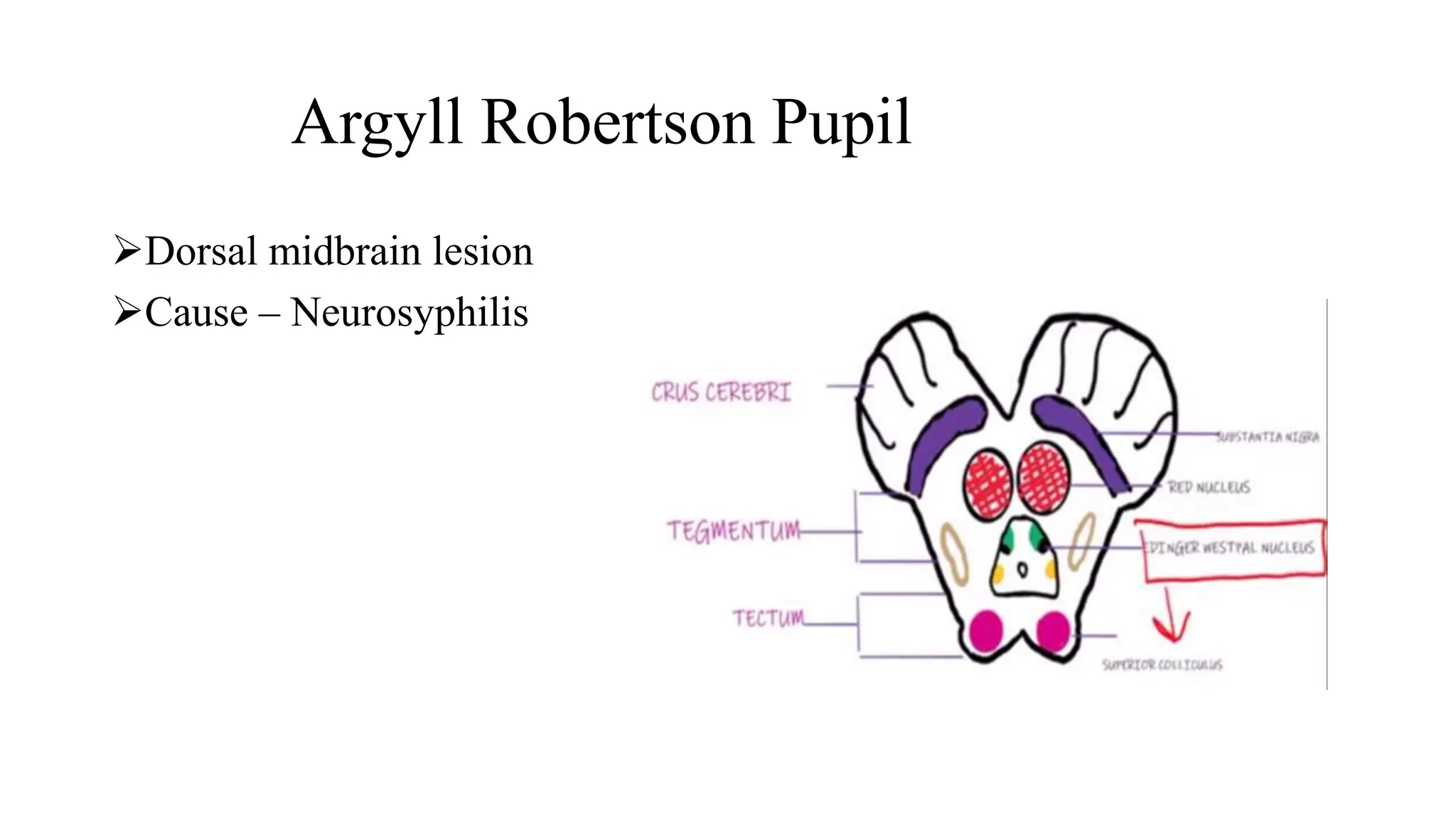
The document discusses various pupillary abnormalities and their underlying pathways, including light reflexes, convergence, accommodation, and sympathetic discharge. It outlines the types of pupillary reflex defects such as total and relative afferent pathway defects, along with conditions like Horner's syndrome and Adie's tonic pupil that affect pupillary reactions. Diagnostic tests and examinations for determining the specific pupillary abnormalities are also described.