1) The pupil forms from the absorption of the central pupillary membrane during development. It regulates the amount of light entering the eye and focuses vision by changing size.
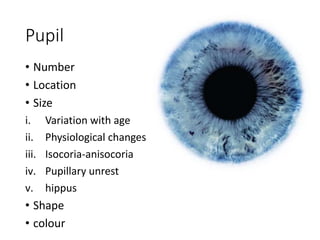
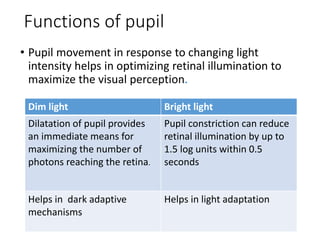
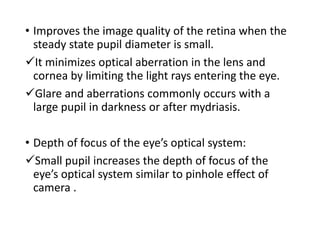
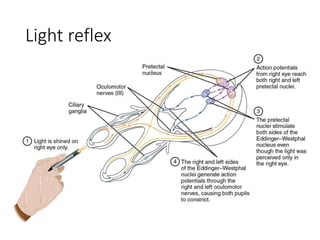
2) The pupil constricts in bright light to reduce retinal illumination and dilates in dim light to maximize photons reaching the retina. Constriction also improves image quality by reducing aberrations.
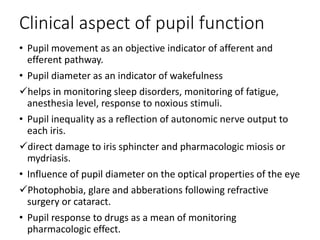
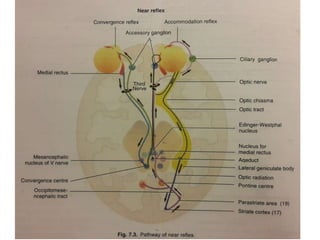
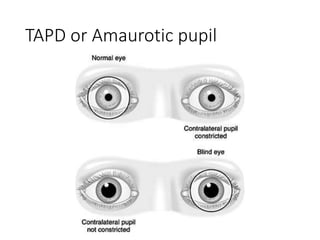
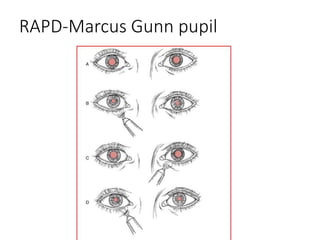
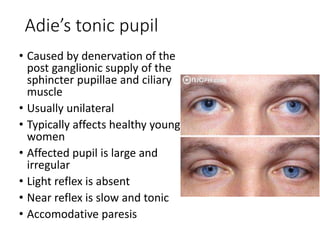
3) Pupillary reflexes include light, near, darkness, and psychosensory reflexes. Abnormalities can indicate lesions in the afferent or efferent pathways. Tonic pupils are caused by damage to the ciliary ganglion and show slow, sustained constriction to light and near stimuli.

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




