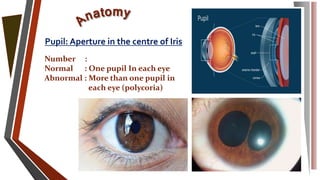
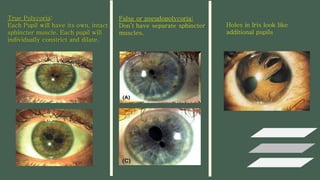
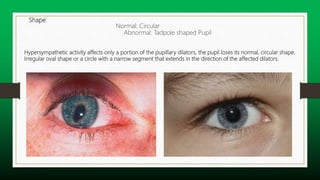
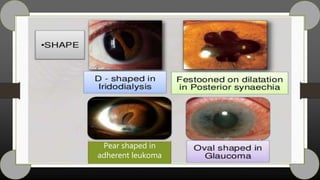
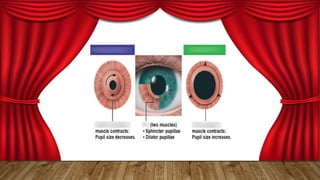
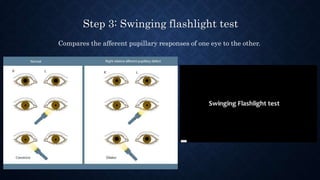
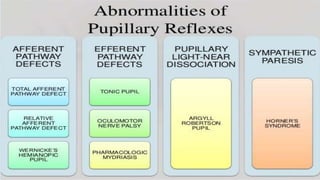
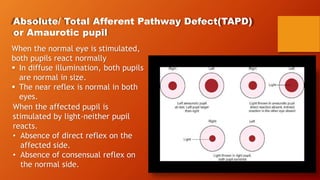
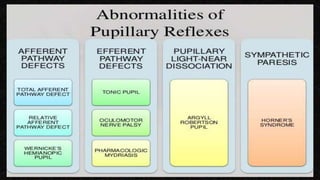
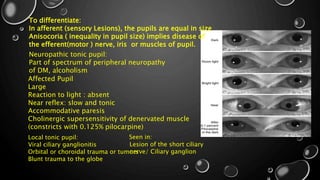
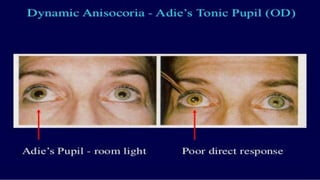
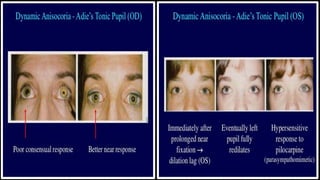
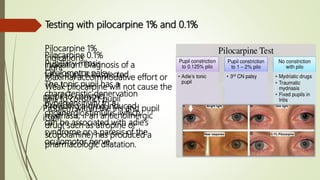
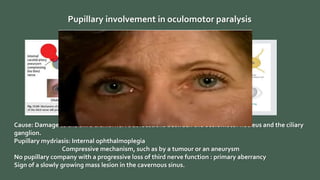
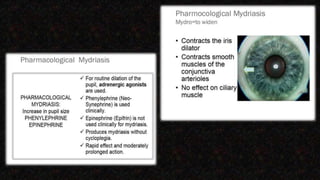
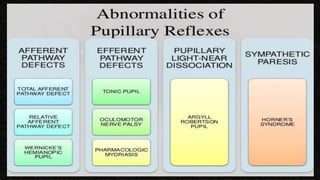
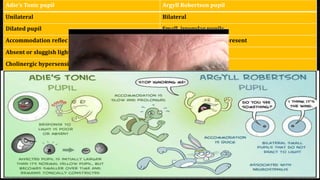
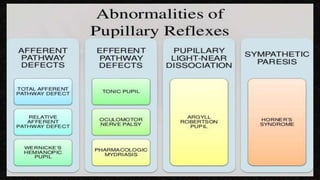
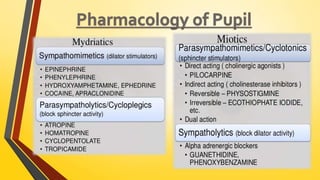
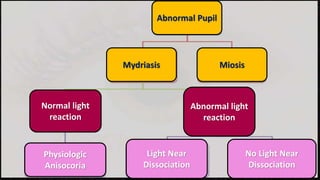
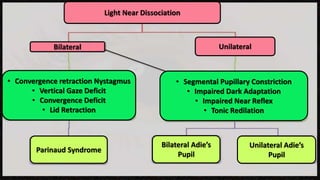
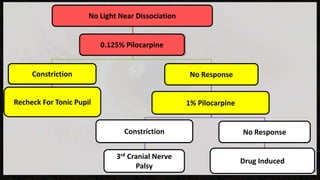
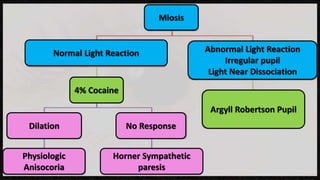
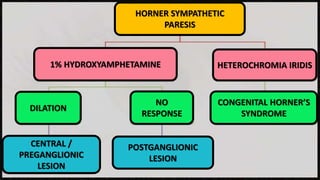
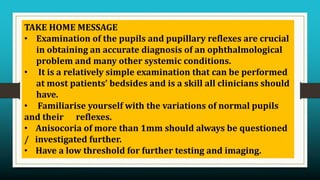
The document discusses the anatomy and physiology of the pupil, including its functions, shape, size, and reflexes. It describes how to examine the pupils through tests of light reflex, near reflex, swinging flashlight test, and reaction to pharmacologic agents. Key abnormalities discussed include anisocoria, afferent pathway defects, tonic pupils, Adie's tonic pupil, and Horner's syndrome. The document emphasizes the importance of a systematic approach to pupil examination and provides tips for optimizing the evaluation of pupillary function and detection of disorders.