Downloaded 544 times

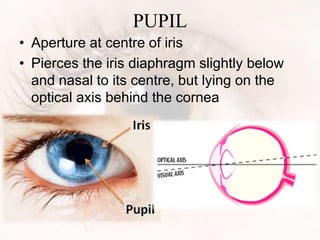
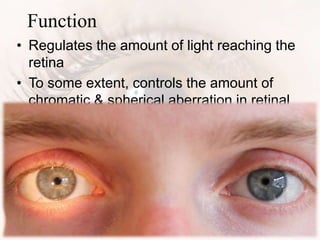

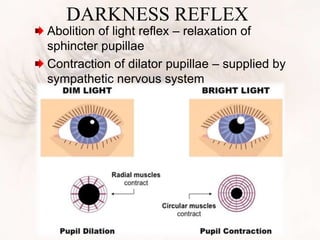
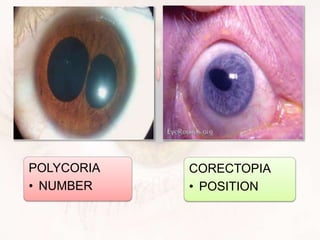
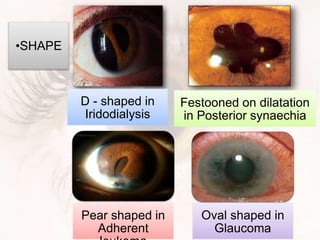

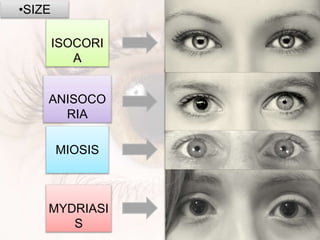
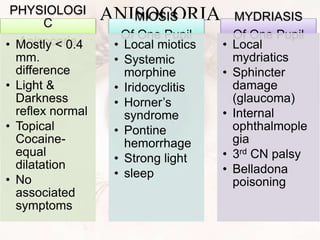
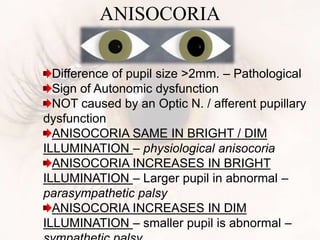
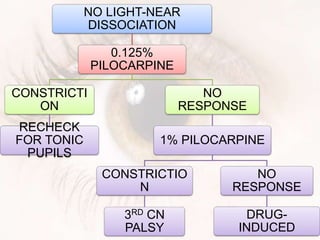
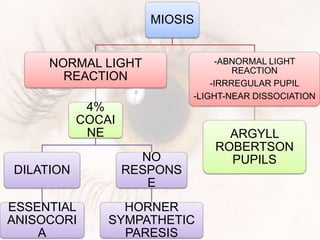
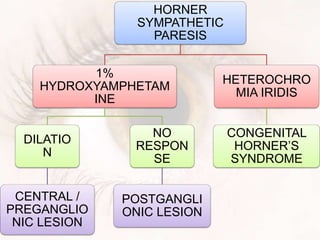


1. The pupil is a circular opening located in the center of the iris that regulates the amount of light entering the eye. 2. Pupil size and reaction are controlled by two sets of muscles - the sphincter pupillae constricts the pupil in response to light, and the dilator pupillae dilates the pupil under sympathetic stimulation. 3. Abnormalities in pupil size, shape, reaction to light and near response can indicate underlying pathologies affecting the complex neurological pathways and muscles that control the pupil. Assessment of pupillary reflexes is important for localizing lesions in the afferent visual pathways or efferent autonomic pathways.


















































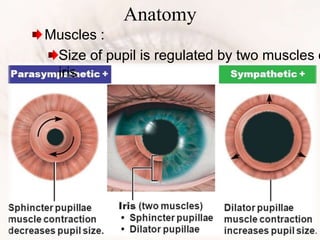
![ANIMAL_CELL_,_TISSUE_AND_ORGAN_CULTURE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animalcelltissueandorganculture1-260204172026-4462b440-thumbnail.jpg?width=640&height=640&fit=bounds)
















