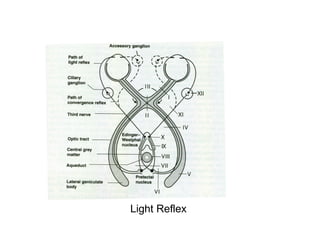
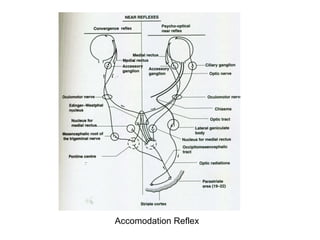
The document discusses the anatomy and physiology of pupillary pathways and their associated reflexes, including the light reflex, accommodation reflex, and various pupillary reactions linked to different medical conditions. It covers the roles of parasympathetic and sympathetic innervation in pupil constriction and dilation, as well as abnormalities such as Marcus Gunn pupil and Argyll Robertson pupil. The importance of these reflexes and reactions as diagnostic clues in ocular and neurological assessments is emphasized.