This document discusses the anatomy and physiology of the pupil and its innervation. It covers topics like:
- The muscles that control the pupil (sphincter pupillae and dilator pupillae) and their innervation.
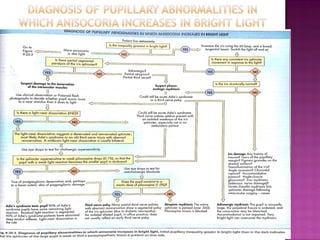
- Causes of anisocoria (unequal pupil size) like drugs, trauma, and neurological conditions.
- Horner's syndrome which causes ptosis, miosis, and anhidrosis due to interruption of the sympathetic pathway.
- Adie's tonic pupil which shows a paradoxical constriction to light and dilation with accommodation due to damage to the parasympathetic pathway.
- Third nerve palsy which can cause ptosis, diplo








![ Difference between the size of two pupil.
TYPE OF ANISOCORIA
1.PHYSIOLOGIC ANISOCORIA:-
1. Simple/central/essential
2. Minimal anisocoria [<0.4mm]
3. Both pupils react well to light
4. No dilatation lag
5. Isolated condition](https://image.slidesharecdn.com/anisocoria-171218135831/85/Anisocoria-10-320.jpg)