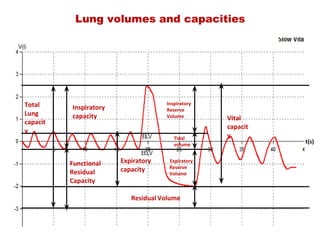
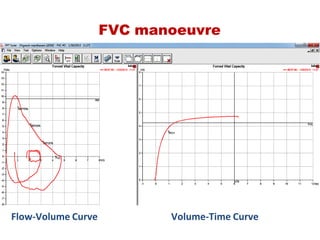
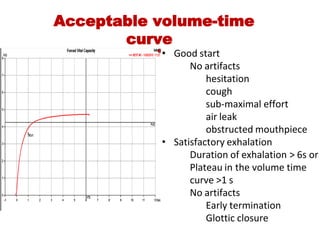
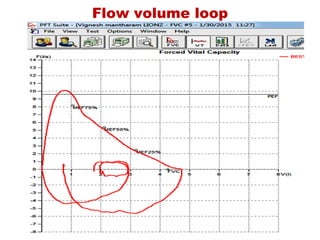
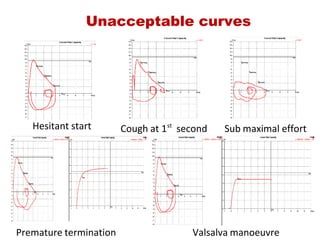
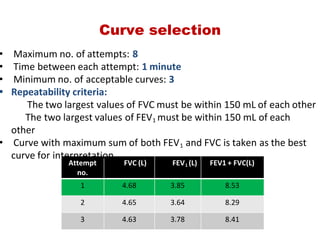
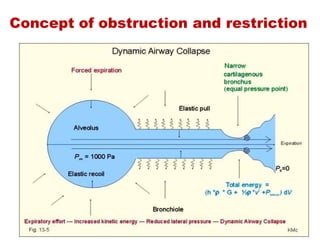
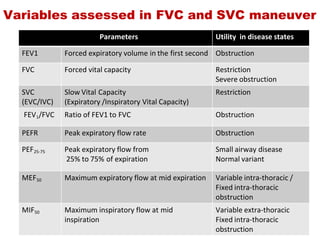
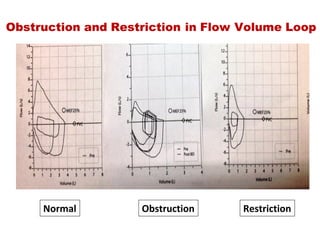
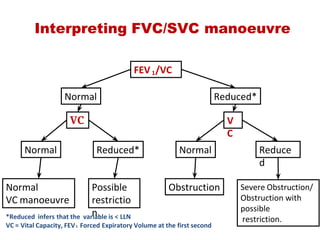
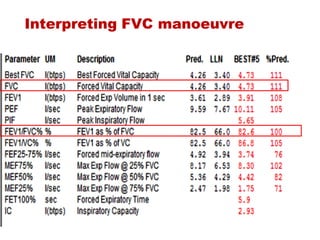
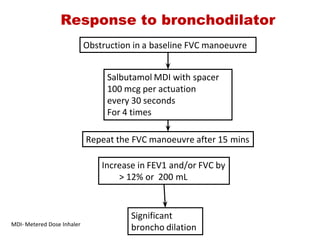
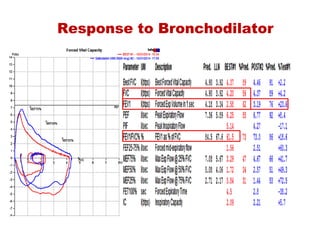
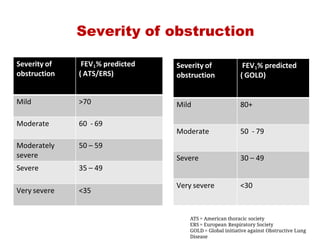
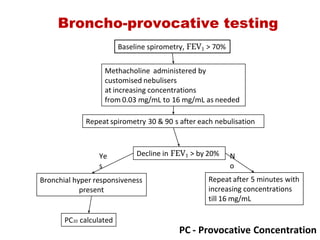
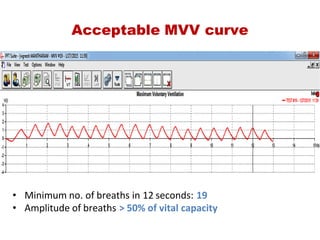
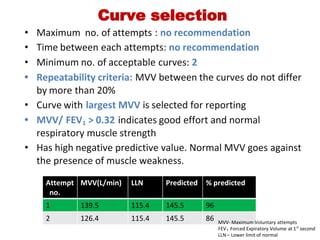
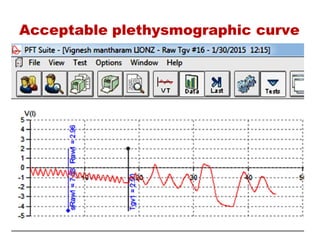
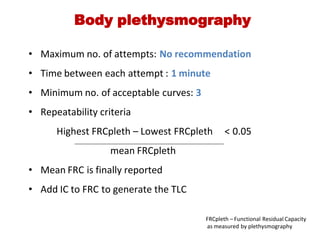
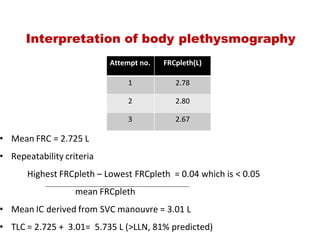
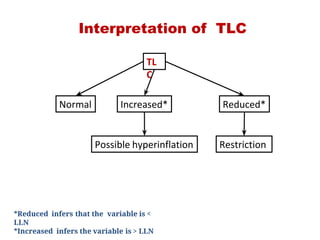
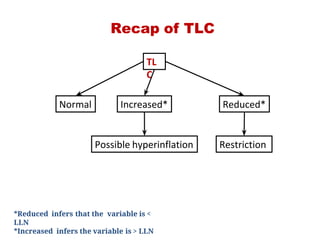
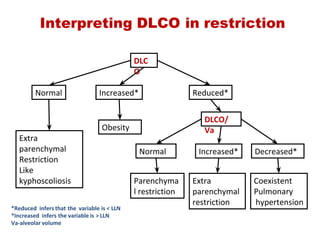
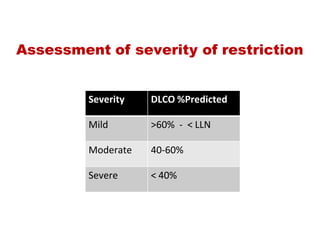
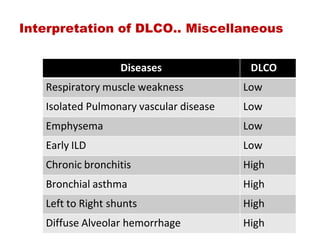
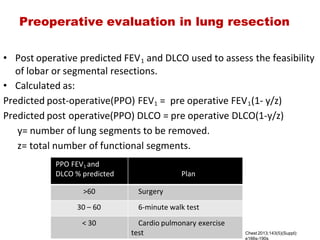
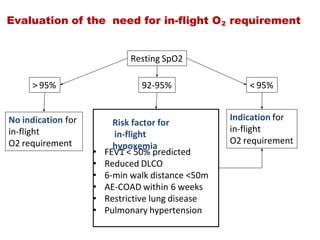
This document provides an overview of pulmonary function testing (PFT). It discusses the history, indications, pre-test evaluation, lung volumes and capacities, specific PFT maneuvers including slow vital capacity (SVC), forced vital capacity (FVC), maximum voluntary ventilation (MVV), and bronchoprovocation testing. Key points covered include acceptable criteria for PFT curves, interpreting results to identify obstruction and restriction patterns, and assessing severity of obstruction. The document is intended to train residents on understanding and performing PFTs as well as interpreting results.