Downloaded 160 times
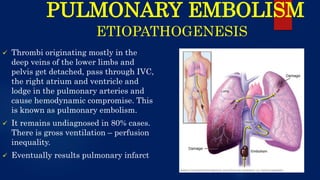
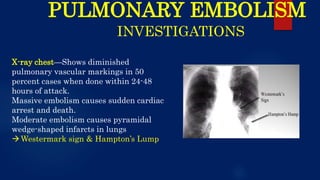
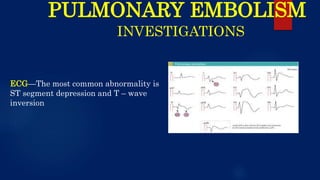
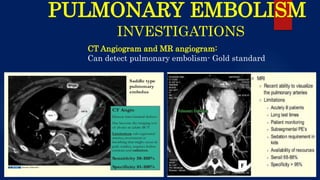
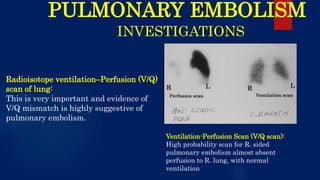
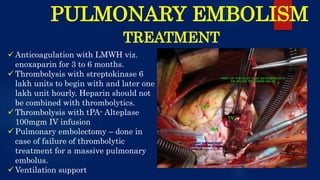


The document provides a comprehensive overview of pulmonary embolism, detailing its etiopathogenesis, which involves thrombi detaching from deep veins and obstructing pulmonary arteries. Clinical features include a triad of dyspnea, chest pain, and hemoptysis, with a range of symptoms from sudden collapse to progressive breathing difficulties. Investigations such as CT angiography and V/Q scans are essential for diagnosis, while treatments include anticoagulation, thrombolysis, and embolectomy in severe cases.










![Acute heart failure [MBBS]](https://cdn.slidesharecdn.com/ss_thumbnails/acuteheartfailure-170323061012-thumbnail.jpg?width=640&height=640&fit=bounds)



























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

