Downloaded 579 times
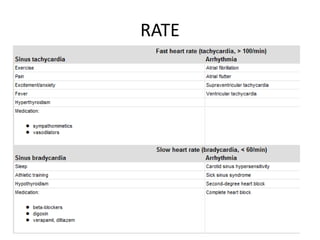
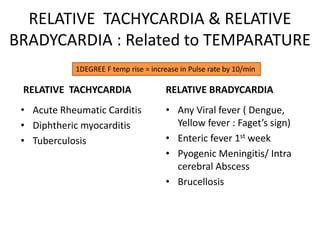
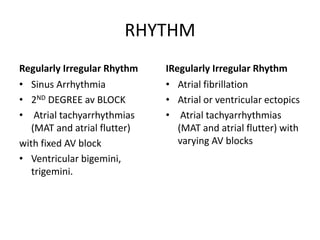
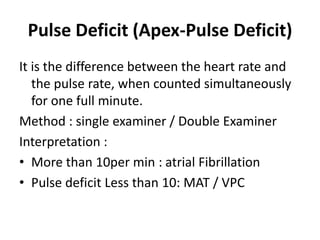
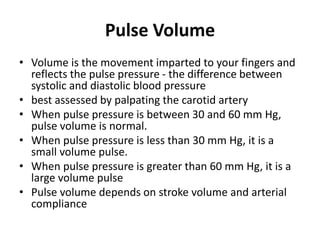
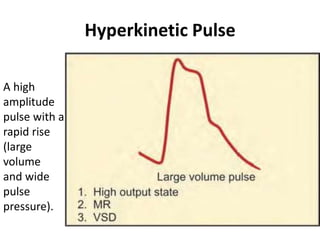

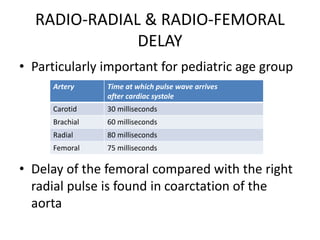


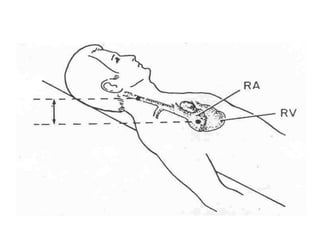

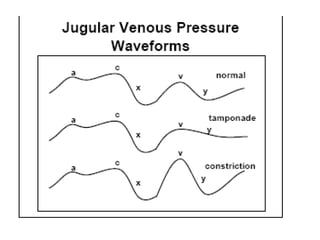
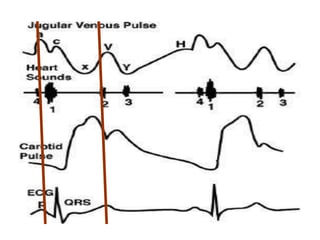
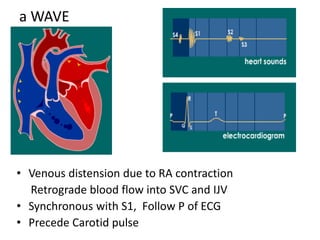
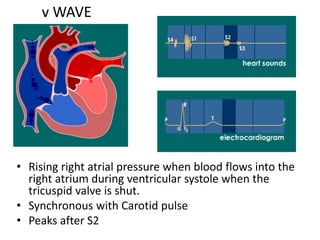
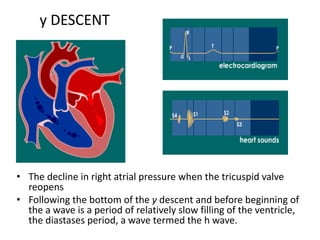
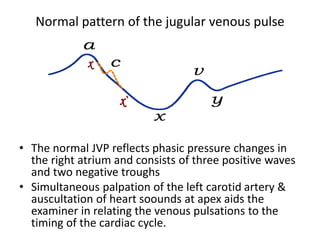
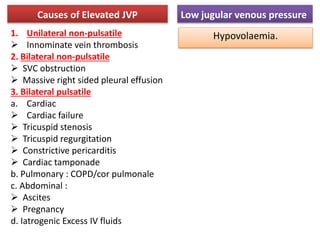
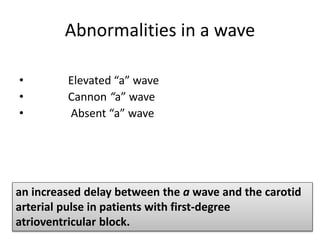
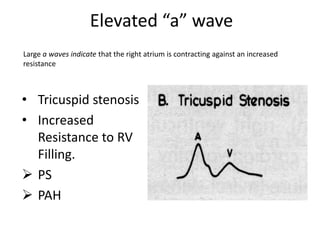
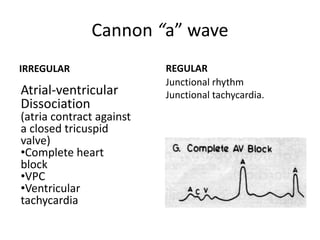
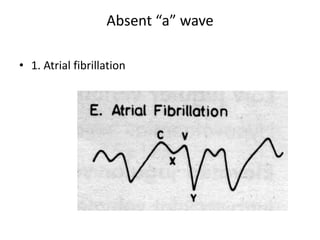


The document provides a review of examining pulse and jugular venous pressure (JVP). It defines pulse as the expansion and elongation of the arterial wall due to blood pressure, and JVP as the oscillating top of blood in the right internal jugular vein reflecting right atrial pressure changes. When examining pulse, the rate, rhythm, volume, character, arterial wall condition, and peripheral pulses are assessed. Abnormal rhythms and characteristics like pulsus paradoxus are also described. Examining JVP involves observing the pressure level and waveform pattern. An elevated or changed waveform can indicate cardiac or pulmonary issues. The document outlines how to properly examine both pulse and JVP and interpret the findings.
































![[Int. med] jugular venous pressure from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/ttnn2w5hsv594ygpbtvp-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171701-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)

























![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)














