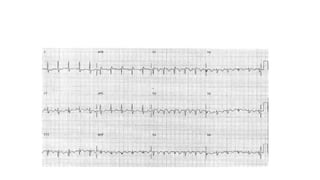
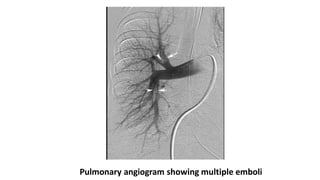
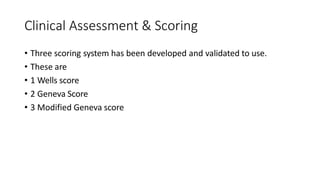
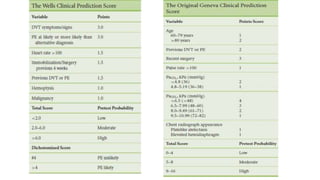
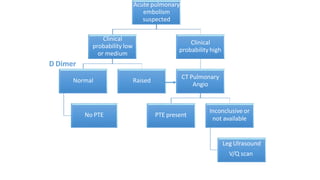
This document discusses pulmonary thromboembolism (PE), which refers to blood clots (thrombi) traveling from deep veins to the lungs. Most clots originate in the lower extremities. Risk factors include inherited conditions, surgery, trauma, immobilization, cancer and pregnancy. PE can cause hypoxemia and pulmonary hypertension. Diagnosis involves clinical assessment, D-dimer testing, chest imaging like CT pulmonary angiogram (gold standard), ventilation-perfusion scanning and echocardiogram. Treatment aims to relieve symptoms and prevent complications like right heart strain.