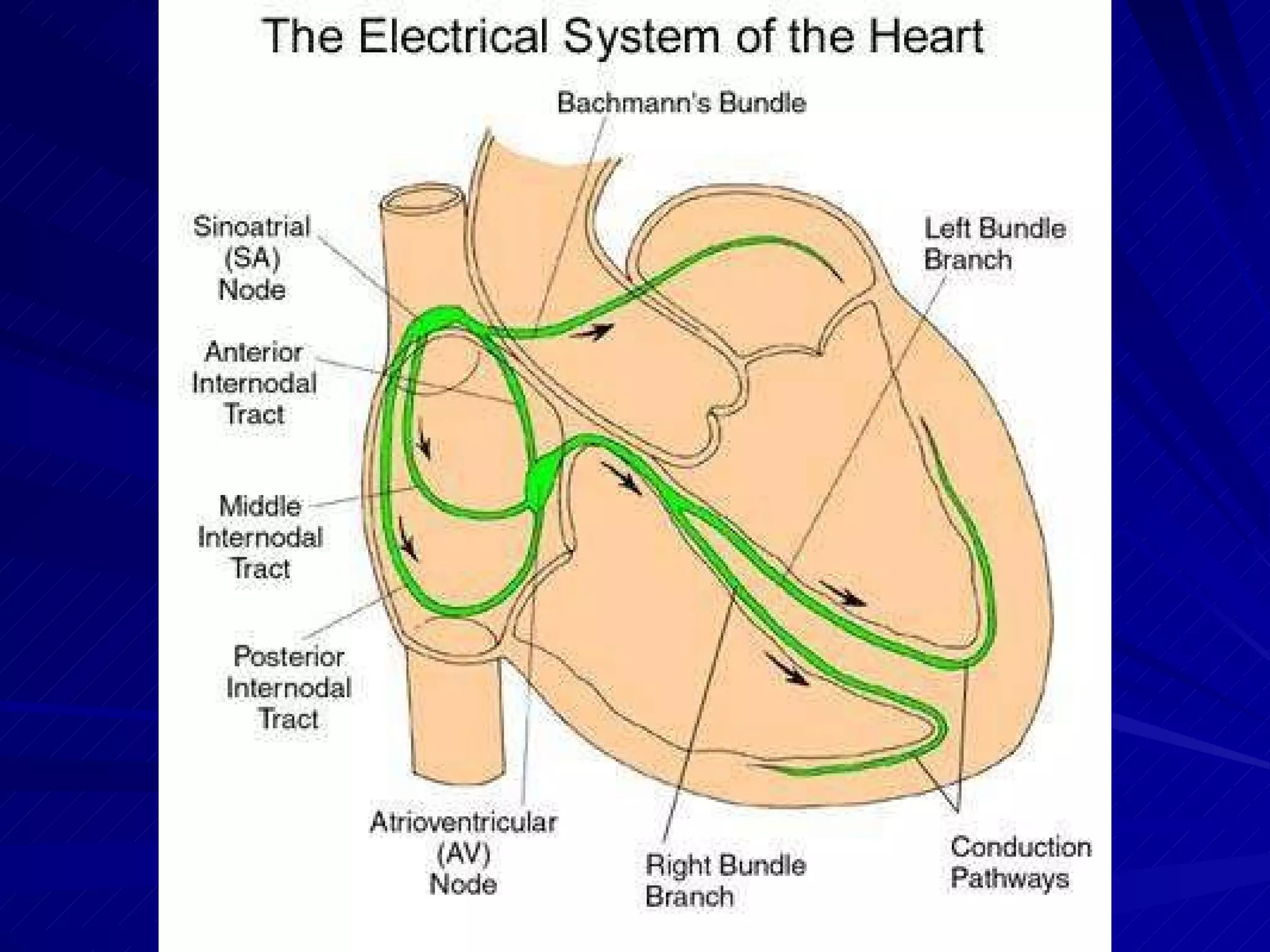
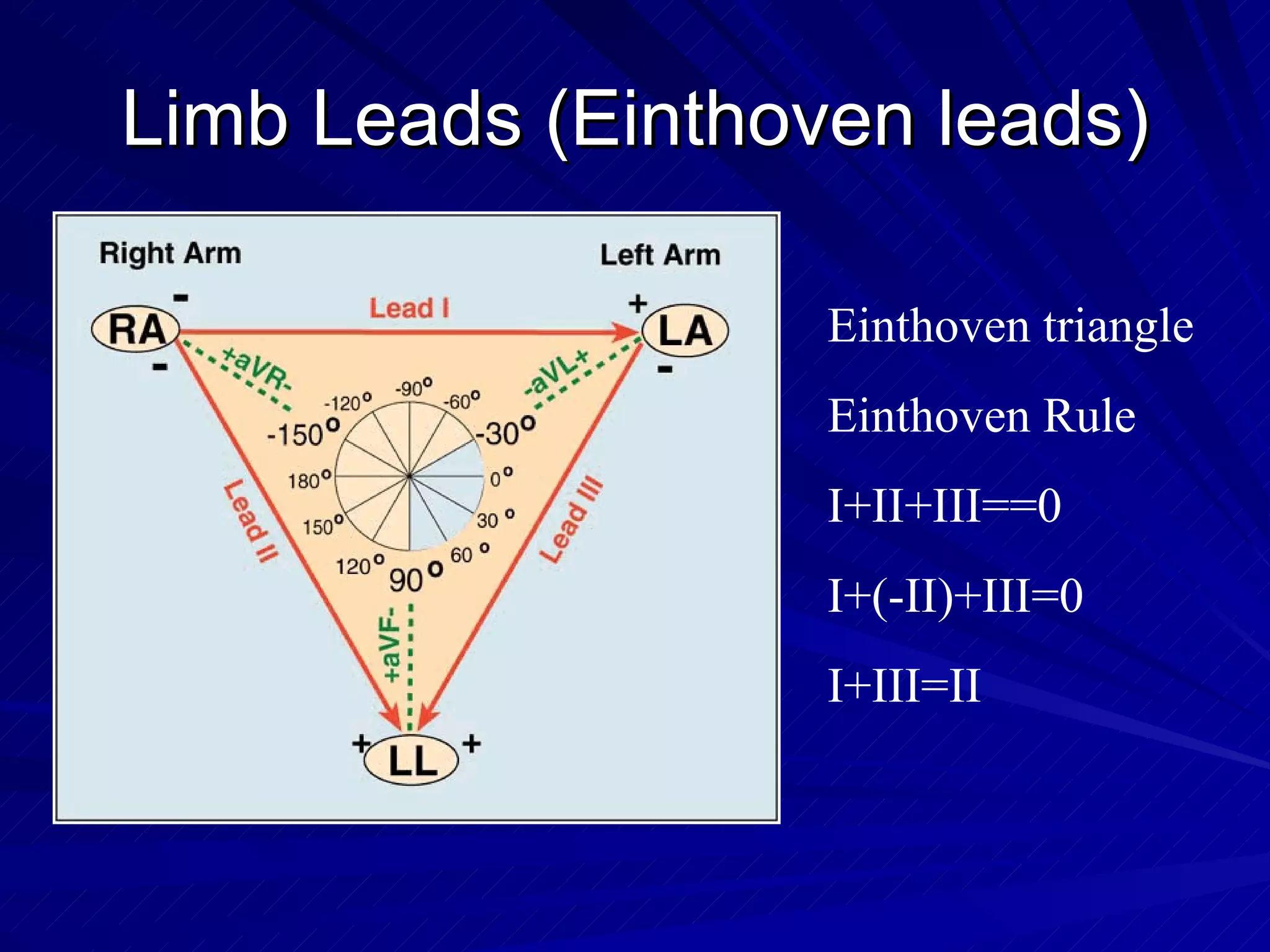
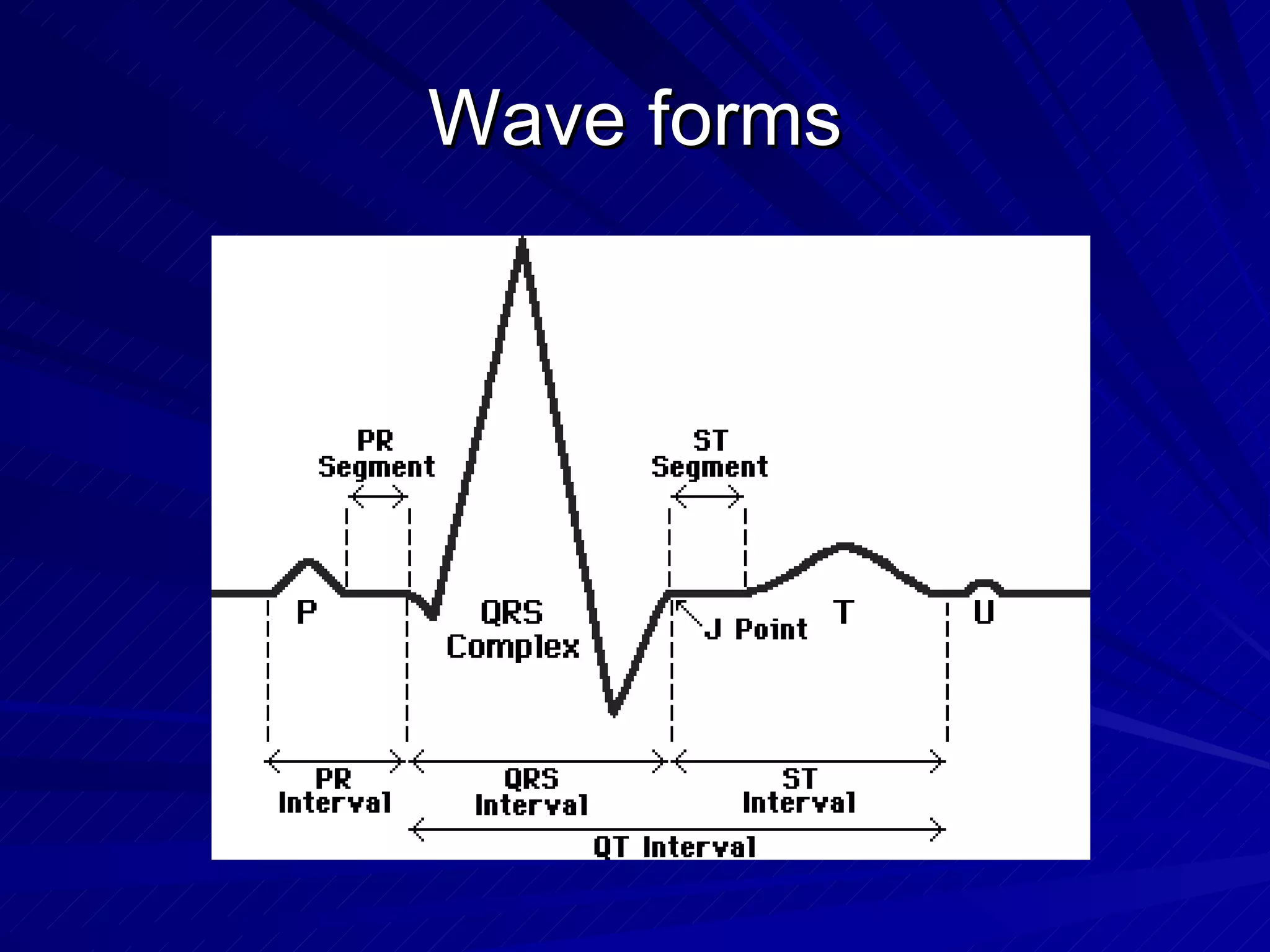
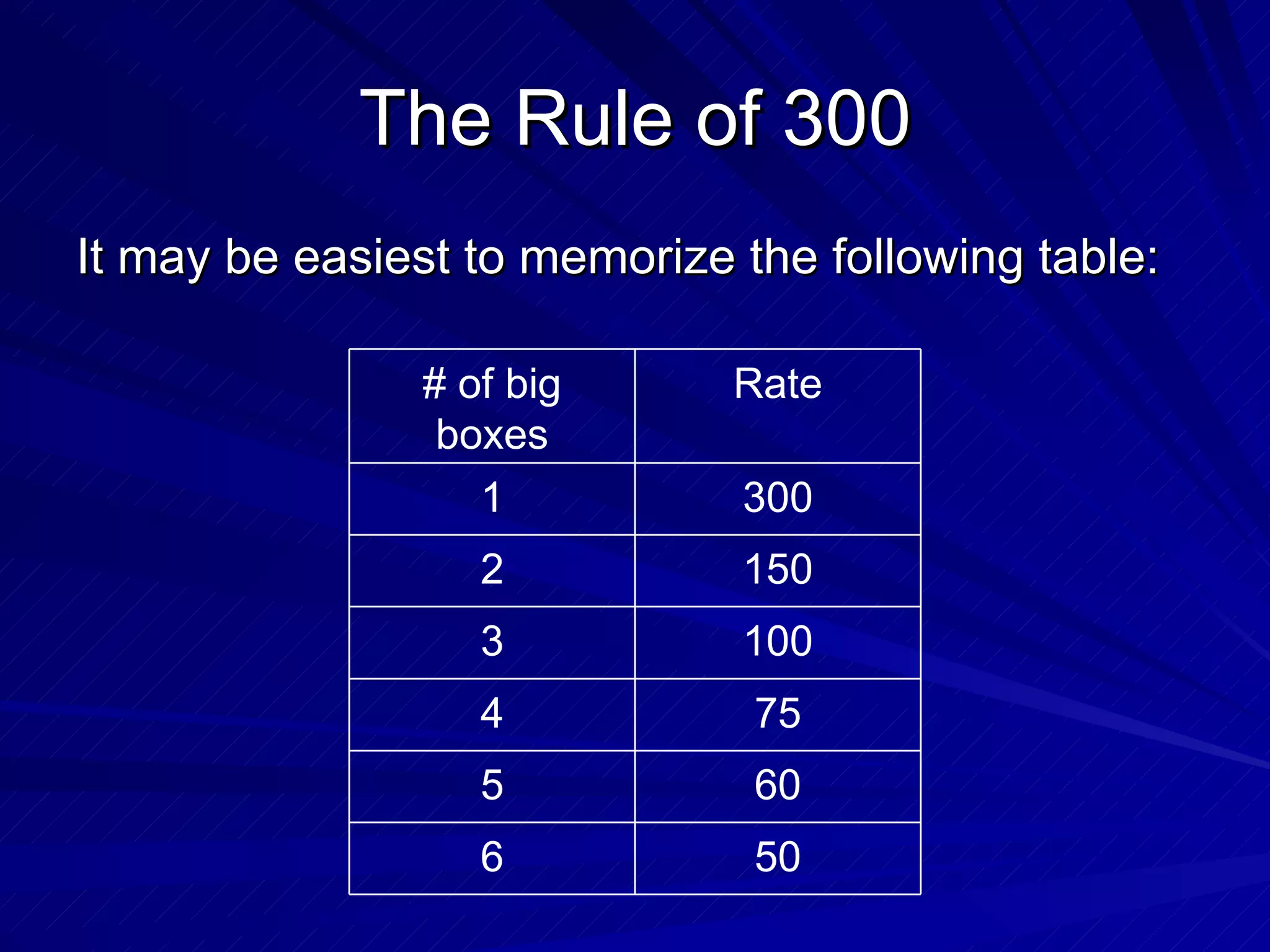
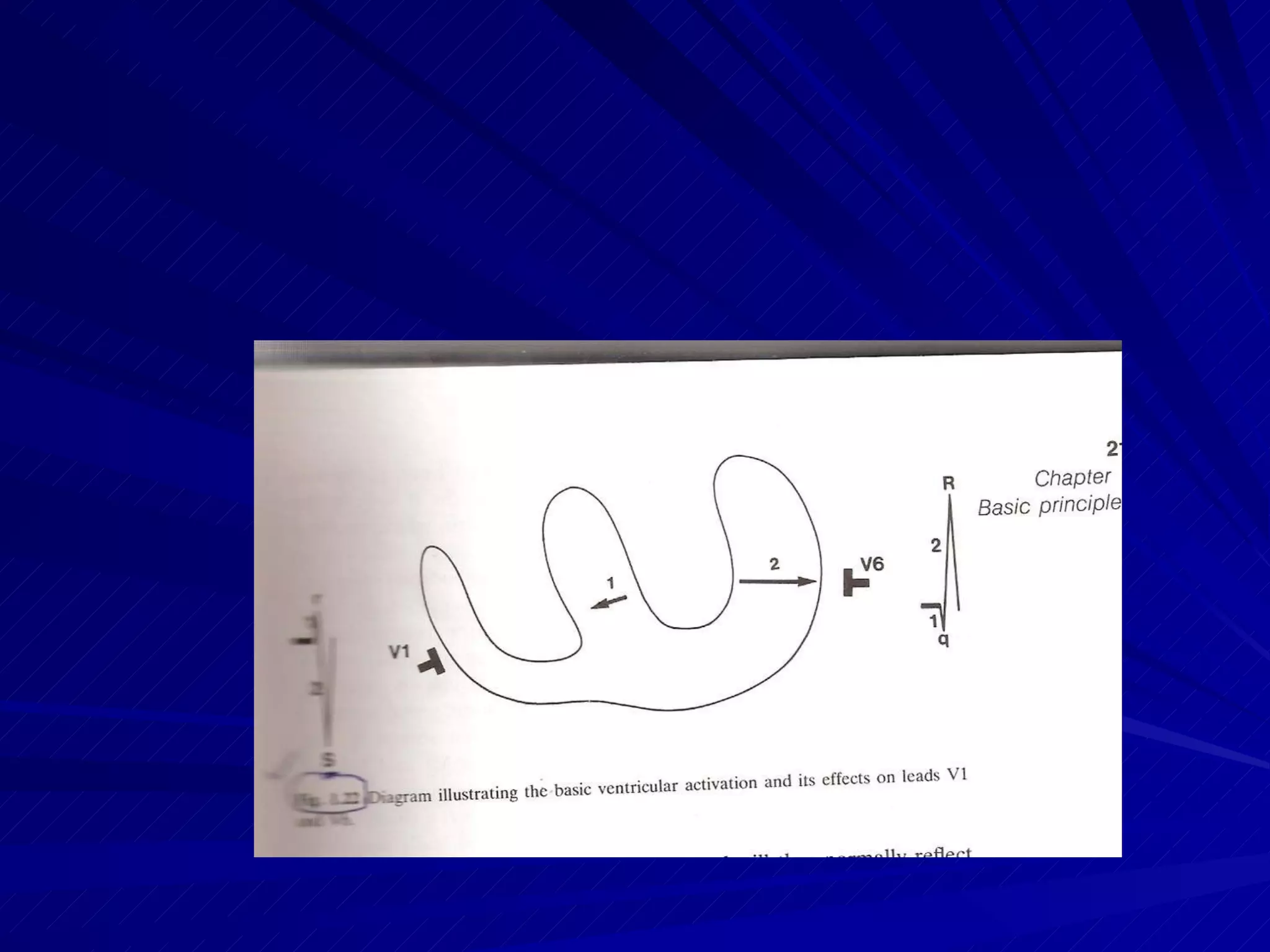
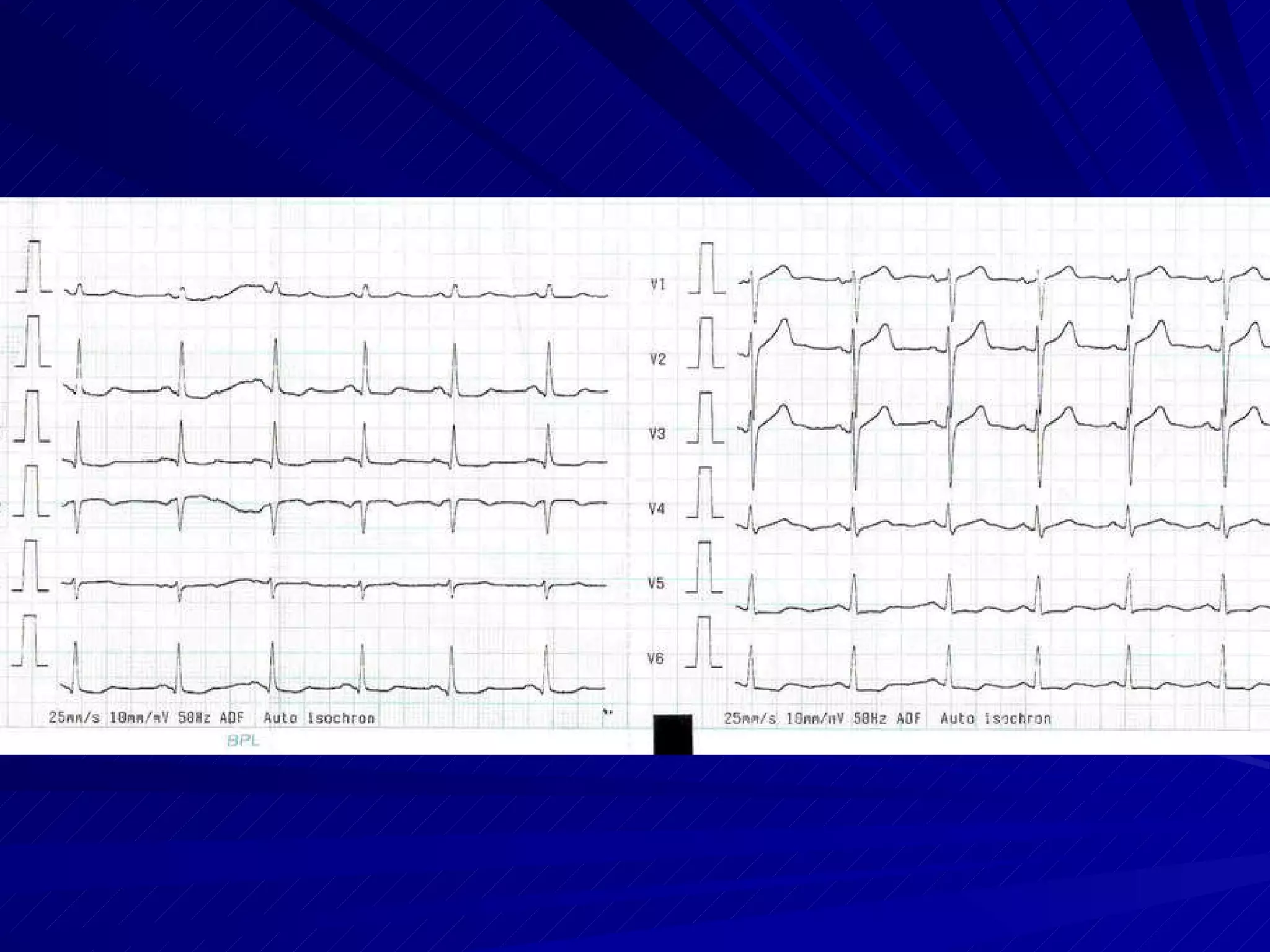
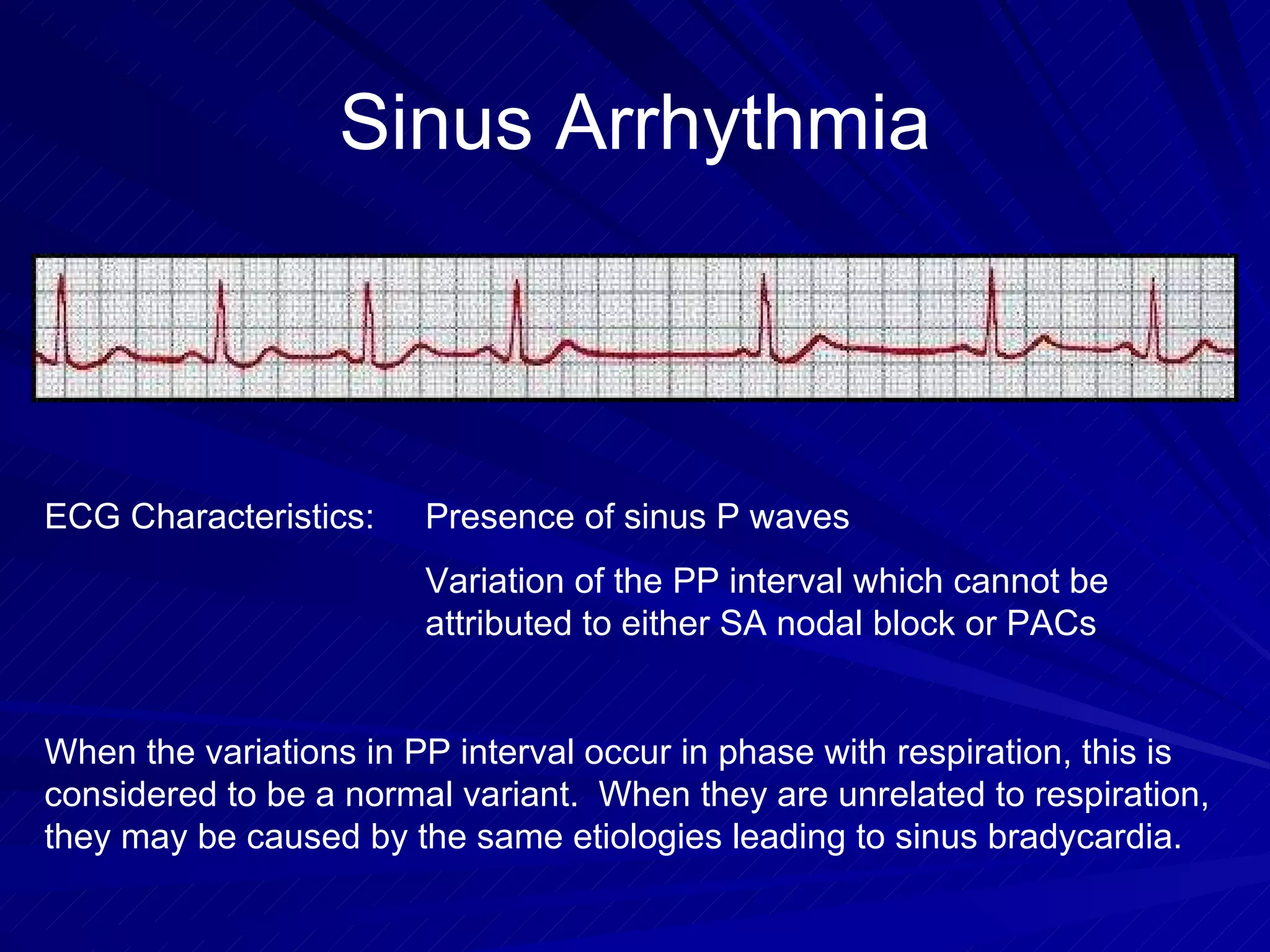
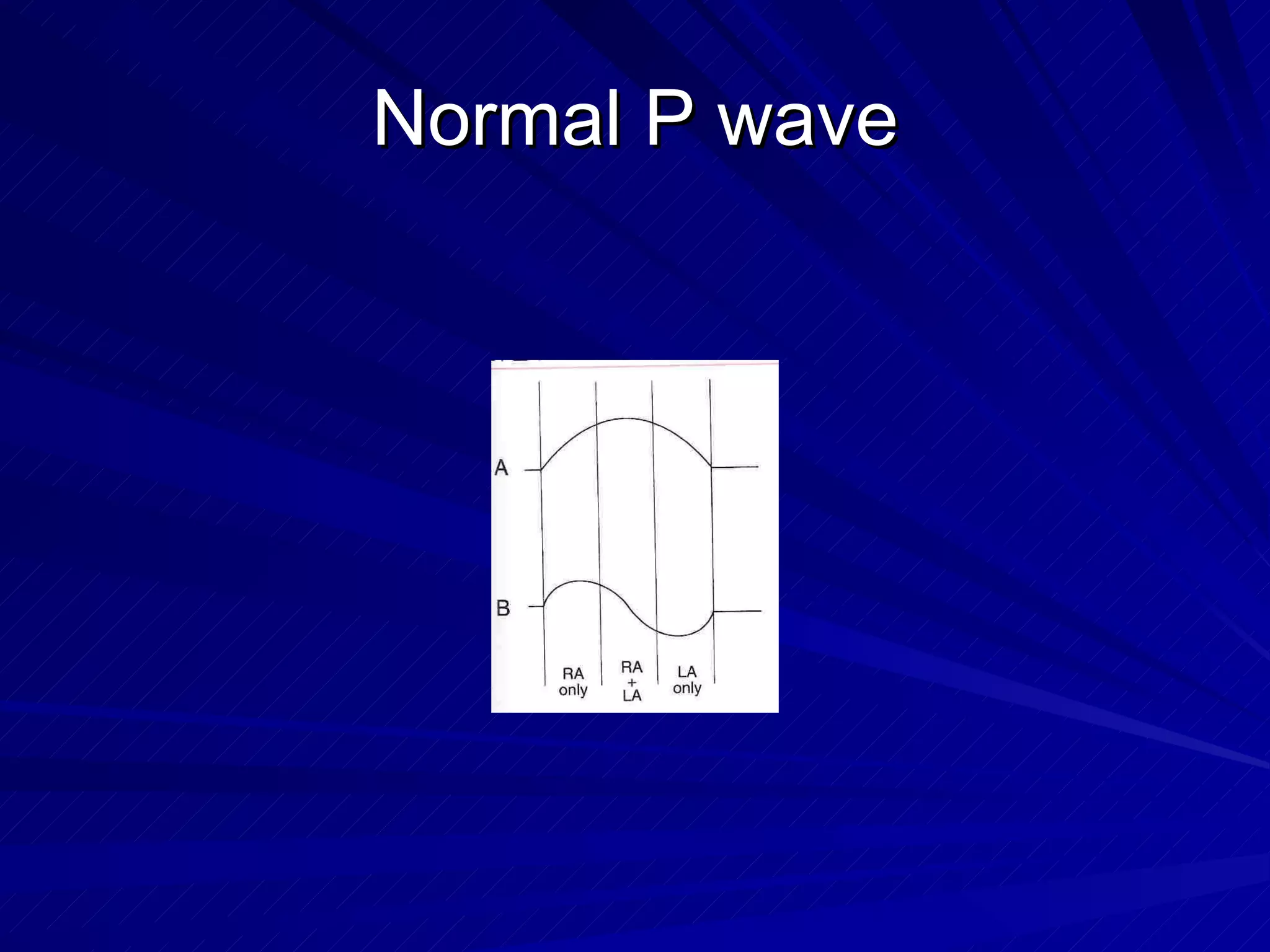
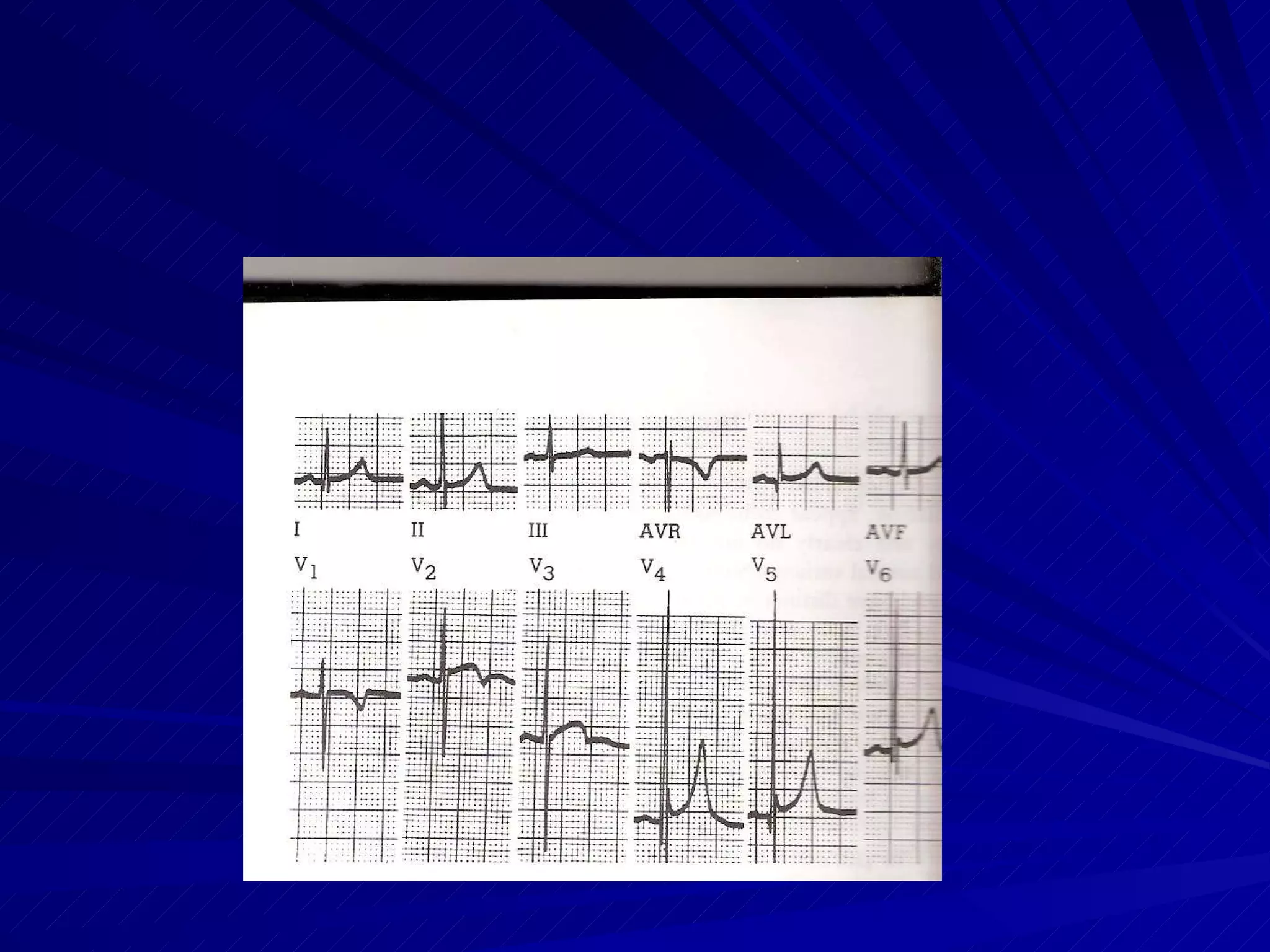
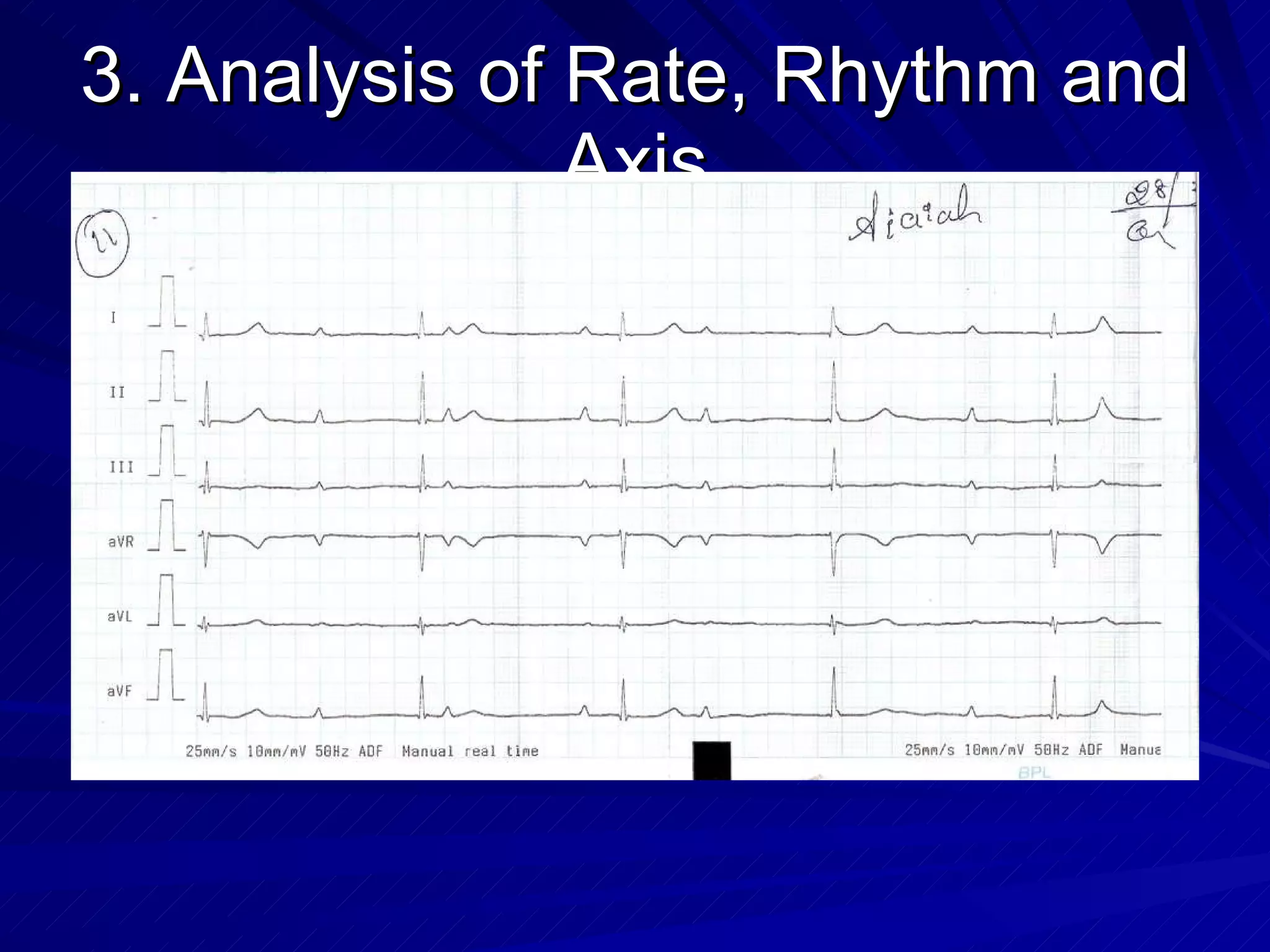
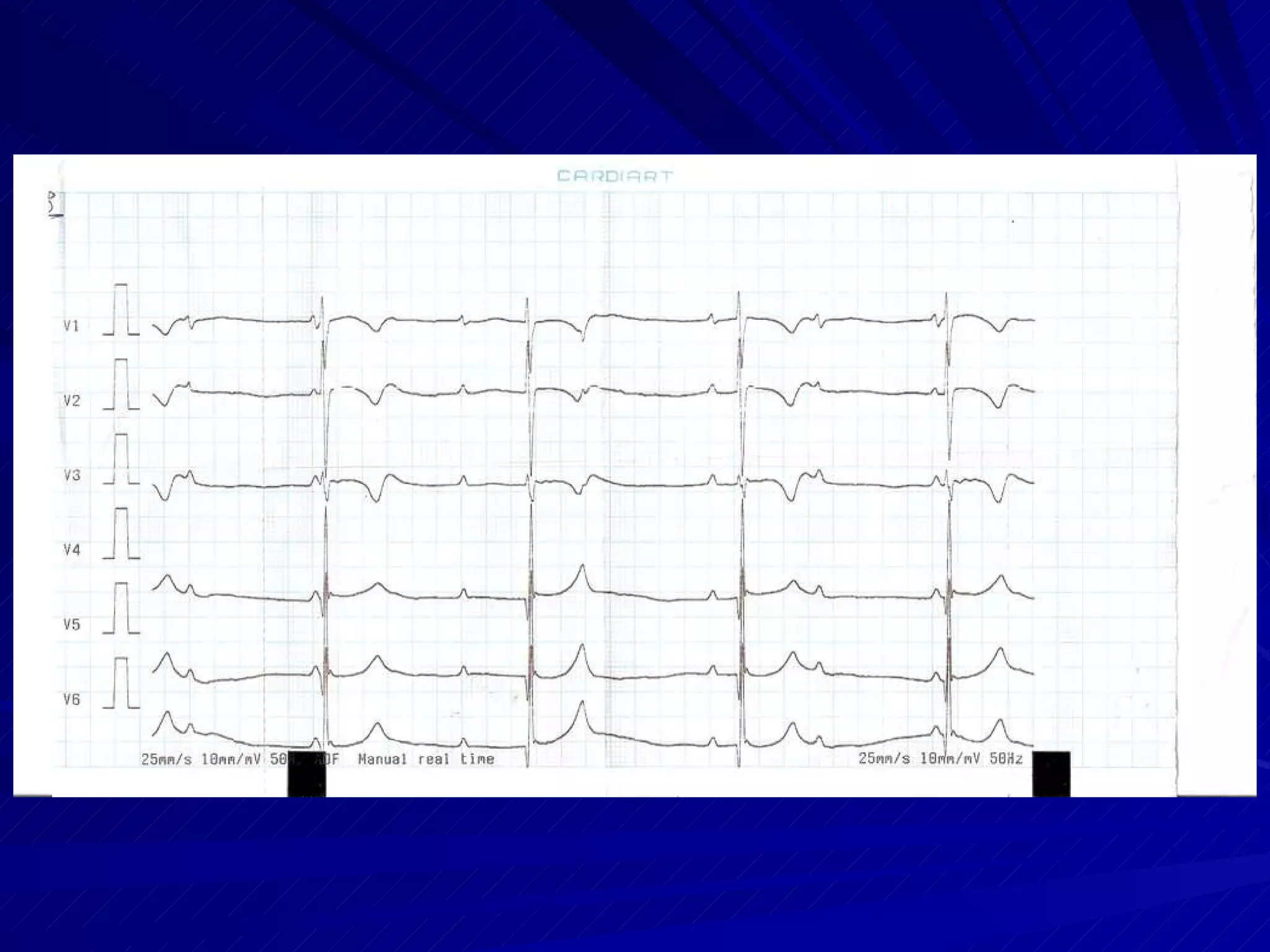
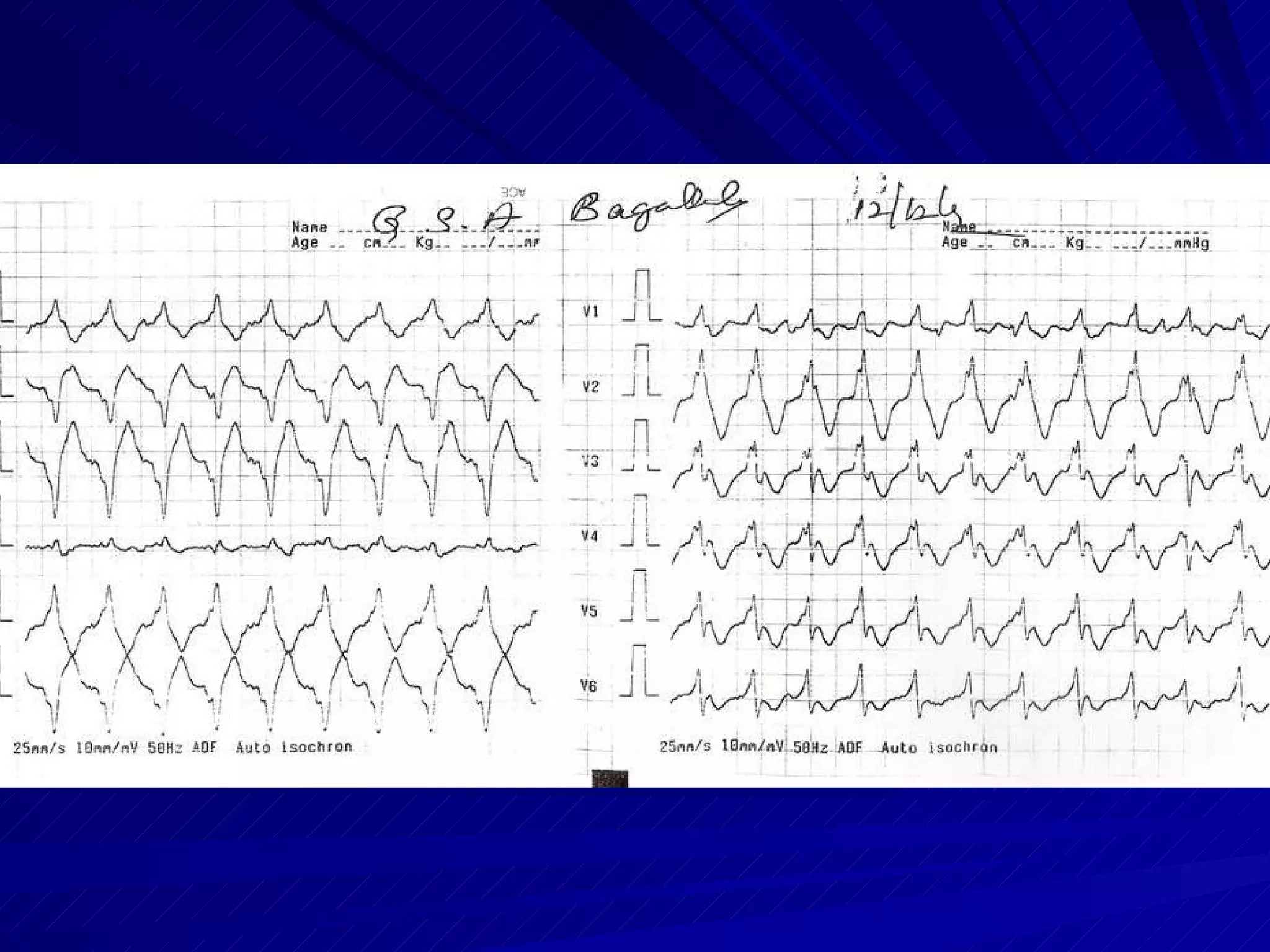
This document provides an overview of electrocardiography (ECG), including how an ECG works, the basics of recording an ECG, ECG leads, normal ECG waveforms and intervals, interpreting an ECG, common abnormalities, and how to report an ECG. It discusses topics such as the cardiac conduction system, Einthoven's triangle, the 12-lead ECG, determining heart rate and axis, normal sinus rhythm, P waves, QRS complex, ST segment, T waves, and the QT interval.