Downloaded 230 times

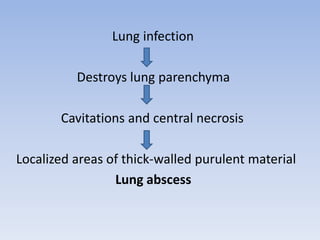
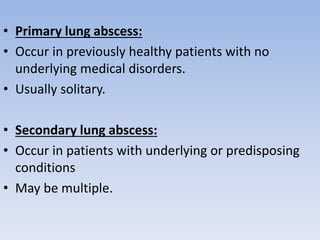
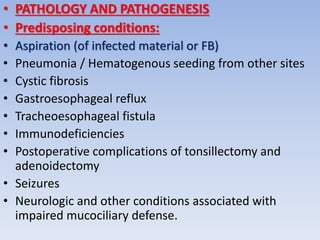
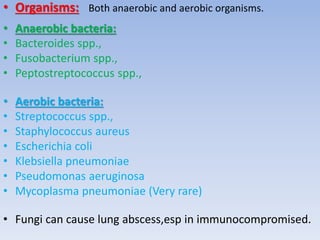

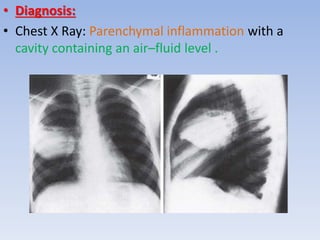
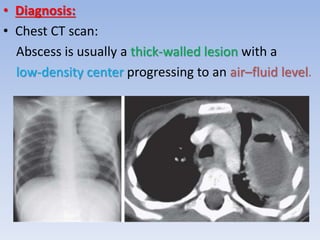


This document discusses pulmonary abscesses in children. It defines a lung abscess as a localized collection of thick-walled purulent material within the lung parenchyma caused by infection and tissue destruction. Lung abscesses can be primary, occurring in previously healthy patients, or secondary, occurring in patients with underlying conditions. Common predisposing factors include aspiration, pneumonia, cystic fibrosis, and immunosuppression. Symptoms include cough, fever, dyspnea, and chest pain. Diagnosis involves chest X-ray and CT scan identifying a cavity containing air-fluid levels. Treatment consists of antibiotics for 2-3 weeks, with surgical drainage for severe or unimproving cases. Prognosis is generally excellent.





































































































