Downloaded 804 times
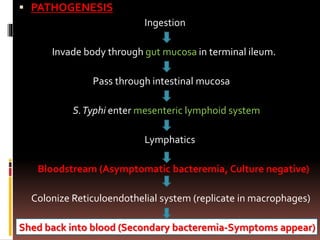

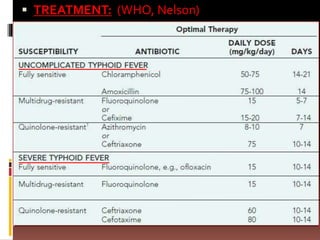
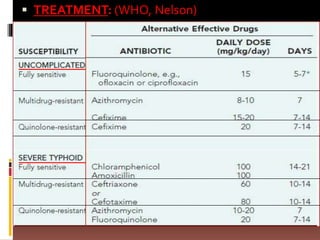




Salmonella enterica serovar Typhi causes enteric fever or typhoid fever in children. It is transmitted through ingestion of contaminated food or water. In the body, it invades the intestinal mucosa and spreads to the bloodstream and reticuloendothelial system. Clinical features include sustained high fever, abdominal discomfort, diarrhea, and complications affecting the nervous, cardiovascular or pulmonary systems. Diagnosis involves blood or stool cultures. Treatment recommended is with third generation cephalosporins like cefixime or ceftriaxone. Vaccines provide protection, especially the Vi conjugate vaccine for younger children.











































































































