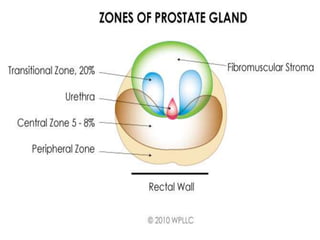
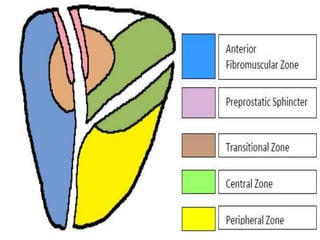
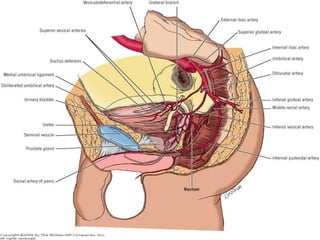
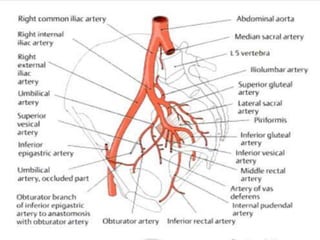
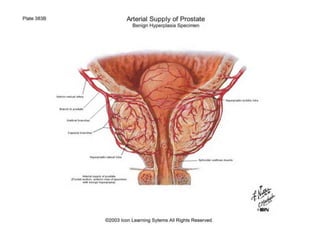
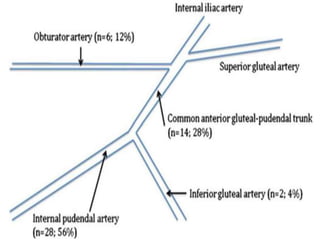
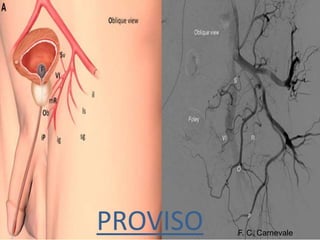
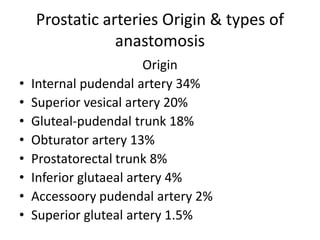
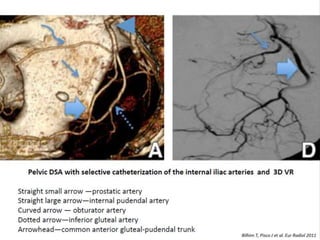
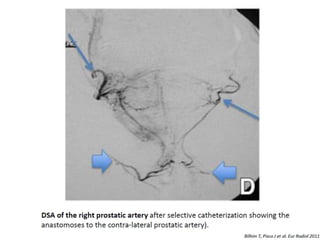
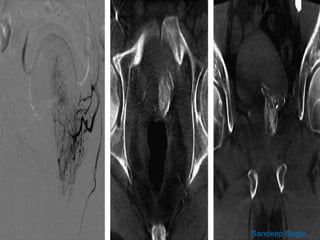
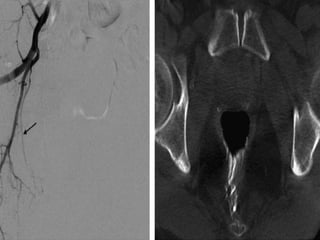
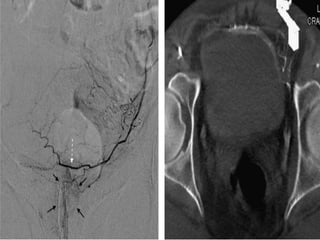
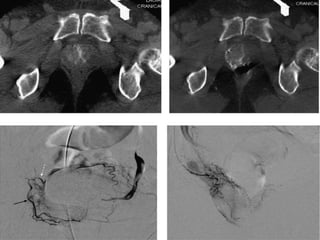
The prostate gland is a pyramid-shaped organ that weighs approximately 20 grams and measures 3x4x2 cm. It has three zones - the peripheral zone (70%), central zone (25%), and transitional zone (5-10%). Prostate cancer develops in the peripheral zone, while benign prostatic hyperplasia (BPH) develops in the transitional zone. The prostate receives its blood supply from various arteries, most commonly the internal pudendal artery (34%). Knowing the detailed arterial anatomy is important for procedures like prostate artery embolization (PAE) to treat conditions like BPH and prostate cancer. Imaging tools like CT angiography and cone beam CT can help the interventional radiologist map the arterial supply before