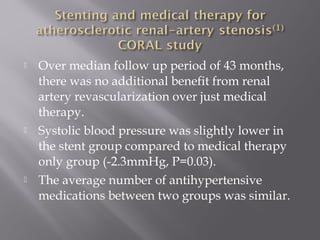
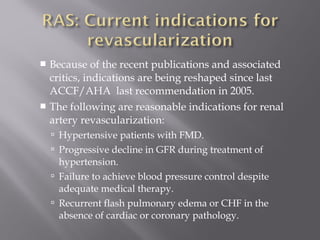
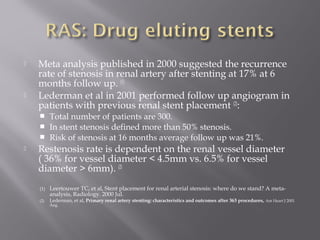
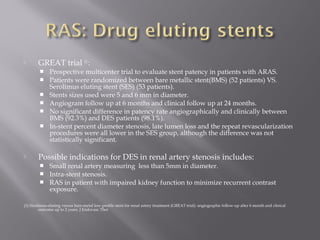
This document discusses renal artery stenosis (RAS), which is narrowing of the renal arteries that can be caused by conditions like atherosclerosis or fibromuscular dysplasia. The two most common causes are atherosclerotic renal artery stenosis and fibromuscular dysplasia. RAS can lead to hypertension, renal impairment, and ischemic nephropathy. While renal artery stenting was often used as treatment, recent clinical trials found no clear added benefits of stenting over medical management alone for atherosclerotic cases. Stenting may still benefit cases of fibromuscular dysplasia or treatment-resistant high blood pressure. The best approach for RAS continues to be evaluated based on ongoing research.















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















