Downloaded 725 times



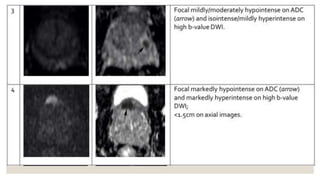
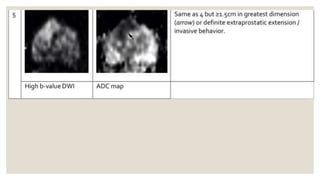

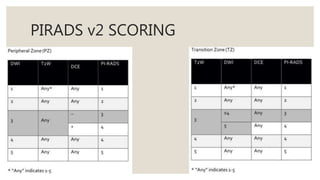
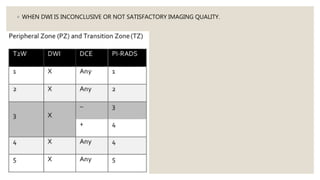
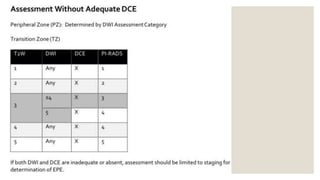









PI-RADS is a structured reporting scheme for evaluating the prostate for prostate cancer using multi-parametric MRI. Version 2 of PI-RADS (PI-RADSv2) was created by a joint committee to standardize terminology and simplify reporting. It aims to improve cancer detection, localization, characterization, and risk stratification. PI-RADSv2 uses T2-weighted imaging, diffusion-weighted imaging, and dynamic contrast-enhanced imaging to assess different areas of the prostate and assigns a score to help determine need for biopsy or treatment. It provides a standardized way to evaluate prostate MRI but has limitations such as not addressing other cancer scenarios or prescribing technical parameters.






























































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)








