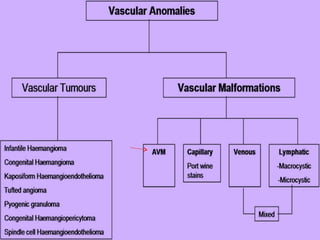
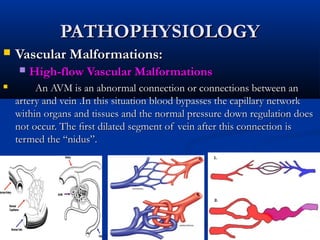
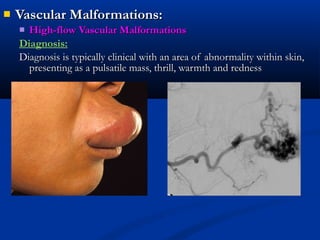
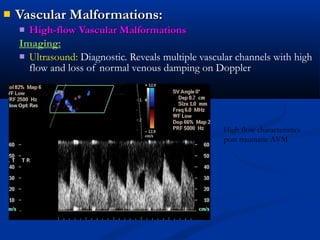
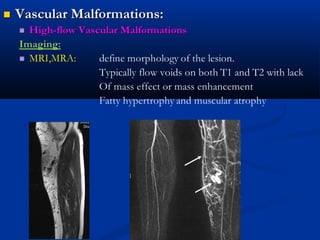
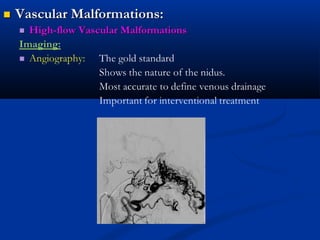
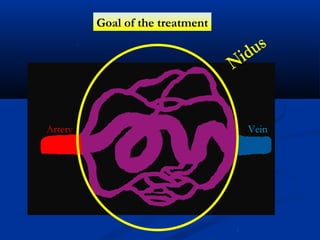
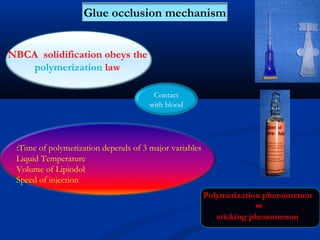
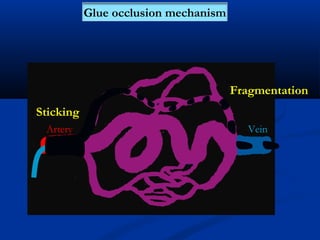
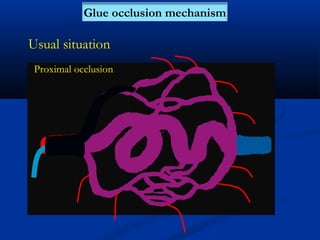
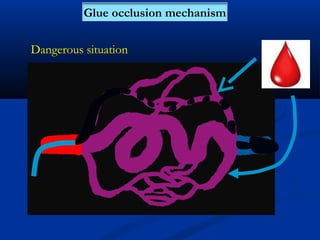
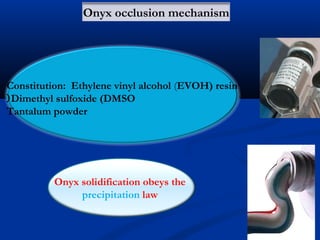
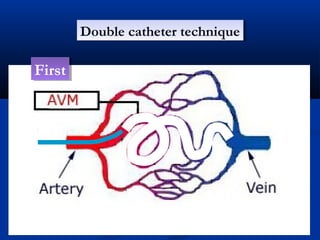
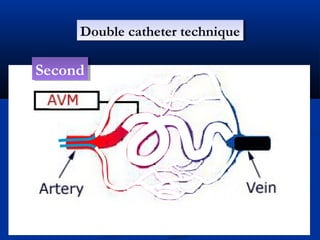
This document discusses the endovascular management of peripheral arteriovenous malformations (AVMs). It defines AVMs as abnormal connections between arteries and veins, bypassing the capillary network. The pathophysiology involves an ectatic capillary bed lacking proper sphincter control. Clinical presentation depends on location and shunting degree, and can include pain, overgrowth, bleeding, and high output cardiac failure in large shunts. Diagnosis is typically clinical and confirmed with imaging showing high flow characteristics. Treatment involves endovascular embolization to occlude arterial feeders using various embolic agents like coils, liquids, and recently the liquid polymer Onyx, which has greater potential to occlude AVMs due to






























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












