Downloaded 185 times
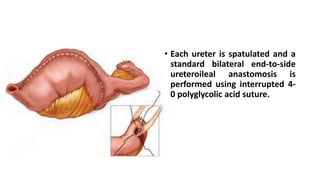
![• The ileal conduit is a technically simple, reliable form of urinary
diversion that became widely accepted and became the gold standard
to which other types of urinary diversion were compared until the
1980s.
• It continues to be by far the most common form of urinary diversion
performed throughout the world today for patients undergoing
cystectomy.
• Long-term complications with the [1970s].
• hyperchloremic metabolic acidosis and
• pyelonephritis were substantially less common than in patients with
ureterosigmoidostomy,](https://image.slidesharecdn.com/orthotopicneobladderfinal-170810182920/85/Orthotopic-neobladder-4-320.jpg)

This document provides an overview of the history and techniques for orthotopic neobladder urinary diversion. Some key points: - Orthotopic diversion was pioneered in the 1950s as an alternative to ureterosigmoidostomy and ileal conduit diversion due to complications of those procedures. - Patient selection considers oncologic factors like risk of urethral recurrence and tumor stage, as well as patient factors like age, renal function, manual dexterity, and prior treatments. - Surgical techniques aim to optimize continence by preserving the rhabdosphincter and its innervation during cystectomy. For males the urethra is detached in a retrograde


![Urinary Diversion after cystectomy [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/urinarydiversionedmond-140716212817-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

























![Muscle invasive bladder Cancer [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/muscleinvasivebladdertumoredmond-140716213247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)















































