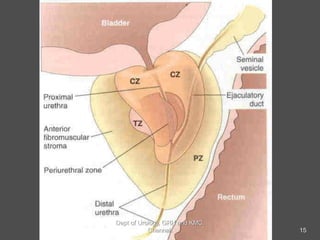
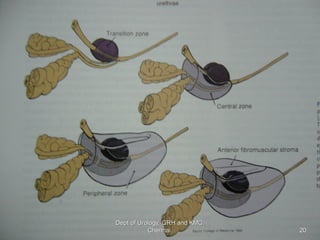
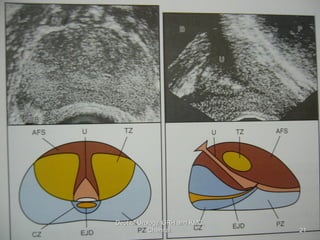
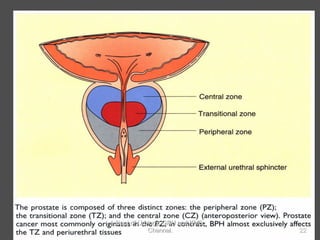
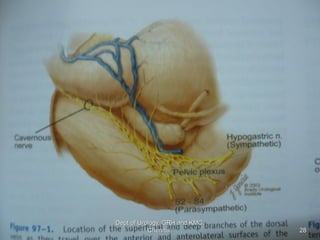
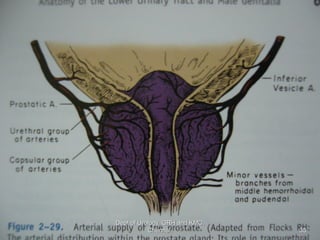
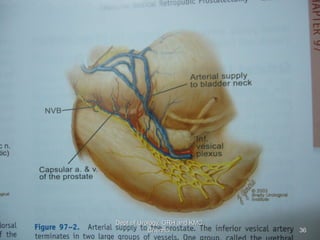
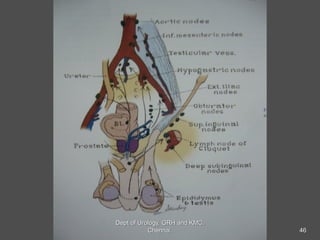
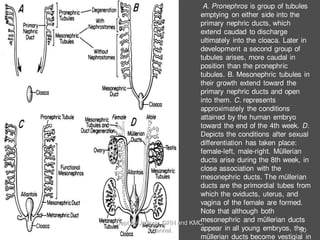
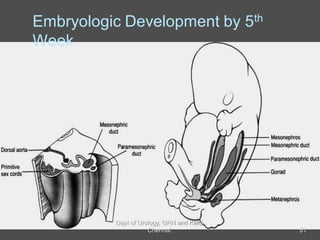
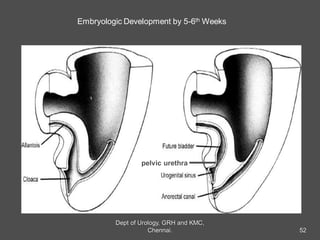
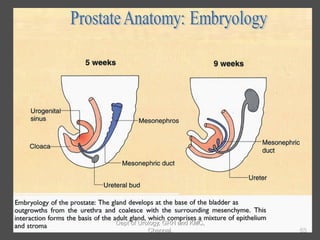
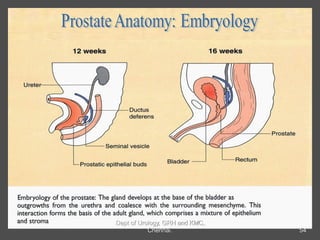
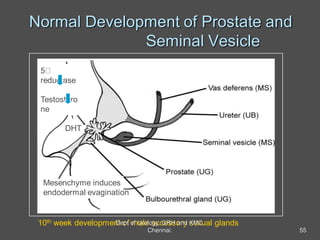
The document discusses the anatomy and embryology of the prostate gland. It describes the prostate's shape, size, surfaces, lobes, capsule, fascia, venous and arterial supply, pelvic plexus, lymphatic drainage and embryological development. The prostate develops from the urogenital sinus in males through androgen-dependent budding and condensation of epithelial cells. Its anatomy includes zones, glandular and fibromuscular composition, and relationship to surrounding structures like the bladder neck.