Presentation1.pptx, radiological anatomy of the petrous bone.
•Download as PPTX, PDF•
53 likes•8,162 views

The document provides an overview of the normal anatomy of the petrous bone, middle ear, and inner ear as seen on radiological imaging. It describes the structures that form the walls and boundaries of the middle ear space, including the tegmen tympani, jugular bulb, and carotid artery. Key structures of the inner ear like the cochlea, vestibule, semicircular canals, and internal auditory canal are also outlined. Various radiographic views used to examine the temporal bone and mastoid air cells are listed. Axial, coronal, and sagittal cross-sections through the temporal bone demonstrate the spatial relationships between the middle ear, inner ear, and surrounding structures.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Presentation1.pptx, radiological anatomy of the petrous bone.
Similar to Presentation1.pptx, radiological anatomy of the petrous bone. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1.pptx, radiological anatomy of the petrous bone.
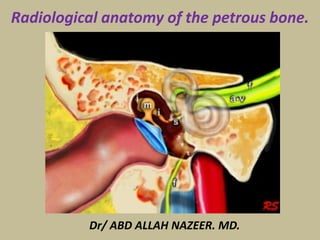
- 1. Dr/ ABD ALLAH NAZEER. MD. Radiological anatomy of the petrous bone.
- 2. Normal Anatomy of the Middle Ear The temporal bone houses and is surrounded by many vital structures. The temporal bone is actually composed of four bones, consisting of the squamous, petrous, tympanic, and mastoid segments. The bony framework of the temporal bone contains multiple air spaces. The most complex of these spaces is the middle ear cavity, or tympanum. The middle ear space is shaped somewhat in the form of a red blood cell stood on end. This space is narrow in a medial-lateral direction and more elongated anteroposteriorly and superoinferiorly. Laterally, the tympanic membrane, annulus, and the handle of the malleus make up the wall of the tympanum. The inner ear forms the medial wall of the middle ear. The largest anatomic structure of the medial wall is the promontory of the cochlea. The roof of the middle ear space is formed by the tegmen tympani. This structure separates the middle ear space from the middle cranial fossa. The tegmen slopes inferiorly as it courses laterally along the temporal bone; remember this point during mastoidectomy to avoid violating the tegmen with the drill. In addition, the tegmen is located higher than the superior border of the tympanic membrane, forming a space, the epitympanum. The epitympanum houses the head of the malleus and the body and short process of the incus.
- 3. The floor of the middle ear is primarily composed of the bone covering the jugular bulb. The bone over the bulb may be dehiscent, rendering it more susceptible to injury. The floor of the middle ear cavity is located further inferiorly than the lowest extent of the tympanic membrane, creating a space, the hypotympanum. Anteriorly and inferiorly, the carotid artery limits the tympanum. More superiorly, the eustachian tube, tensor tympani, and cochleariform process can be observed along the anterior margin of the middle ear. The mastoid air cells lie immediately posterior to the middle ear space. The entrance to the mastoid air cells is the aditus ad antrum. The pyramidal eminence (giving rise to the stapedius tendon) and the incudal fossa can also be observed immediately posterior to the middle ear space. The middle ear space contains several spaces of clinical significance. The sinus tympani is located between the labyrinthine wall and the pyramidal eminence. This area is a common site for recurrence of cholesteatoma. The facial recess is found between the tympanic annulus and pyramidal eminence. This recess provides improved access to the middle ear space during a tympanomastoidectomy.
- 4. Normal Anatomy of the Inner Ear The inner ear is housed in the bony labyrinth, which is well demonstrated on CT scans. The cochlea lies anteriorly. The cochlea is a conical structure, with its apex pointed anteriorly, inferiorly, and laterally; its base rests near the internal auditory canal and extends outward for 2.5-2.75 turns. Immediately anterior to the cochlea is the carotid artery. The round window is located in the scala tympani of the basal turn of the cochlea. The round window niche houses the round window. This window is the termination of the scala tympani of the cochlea. The niche protects the round window from direct exposure to sound waves in the event of a tympanic membrane perforation. The vestibule lies posterior to the cochlea, abutting the internal auditory canal medially. The stapes footplate transmits vibrations to the vestibule at the oval window. The 3 semicircular canals emanate from the vestibule. The lateral canal lies 30° from horizontal. The 3 canals lie at right angles to each other.
- 5. The endolymphatic sac is posteromedial to the semicircular canals on the posterior margin of the petrous bone. The seventh and eighth cranial nerves (CN VII and CN VIII) course through the internal auditory canal. CN VIII enters the structures of the inner ear to innervate them and CN VII passes laterally and anteriorly to the geniculate ganglion, then posteriorly along the medial wall of the tympanum before heading inferiorly to the stylomastoid foramen. A retrospective CT-scan study by Saxby et al found the rate of semicircular canal dehiscence in pediatric patients to be significantly lower than rates found in previous studies. The study involved 334 children (649 temporal bones), with temporal bone imaging revealing superior canal dehiscence in 3.3% of patients (1.7% of temporal bones) and posterior canal dehiscence in 2.1% of patients (1.2% of temporal bones).
- 6. Radiographic positions of mastoids The mastoid process is a part of the temporal bone which is also comprised of tympanic, petrous and squamous parts. Accordingly, examination of the mastoid can be possible using the following projections: Law view: The X-ray beam is directed at a 15 degree oblique plain cephalocaudally while the skull's sagittal plane is parallel to the X-ray film. Law view: The X-ray beam is directed at a 15 degree oblique plain cephalocaudally while the skull's sagittal plane is parallel to the X-ray film.
- 7. Stenver's view: It is also called an Axio-anterior oblique posterior view. The X-ray beam is directed at a 14 degree angle caudally and the head faces the film with slight flexion and rotation at an angle of 45 degrees to the opposite side.
- 8. Transorbital view: (posterioanterior and anteroposterior): The X-ray beam is directed either postero anteriorly or anteroposteriorly along the orbito-meatal line at a 90 degree angle to the film.
- 9. Town's view: It is an anteroposterior view with a 30 degree fronto-occipital axial tilt. It helps in visualization of the temporal bones of, arcuate eminence, mastoid antrum, superior semicircular canal, internal auditory meatus, cochlea and external auditory meatus. It is also valuable in the diagnosis of apical petrositis and acoustic neuroma.
- 10. Axial anatomy from inferior to superior At the most inferior level we see the facial nerve passing inferiorly to finally reach the stylomastoid foramen (not shown in this image). The carotid artery is shown within the carotid canal. Also at this level is the top of the jugular bulb. Coronal anatomy The petrous bone is positioned in an oblique orientation from posterolateral to anteromedial. As a result most structures will be sectioned obliquely on coronal images. The following coronal images go from anterior to posterior. First we will see the tympanic membrane with the ossicles, followed by the cochlea, antrum and semicircular canals. Finally the most posterior image will show the point where the facial nerve exits the temporal bone at the stylomastoid foramen.
- 11. Glenoid fossa Scissura eardrum Fascial canal Mastoid air cells. Occipital condyle Jugular foramen. Foramen magnum Carotid foramen. Tensor tympani
- 12. Fascial canal Jugular foramen. Tensor tympani Eustachian tube Corda tympani canal
- 13. Fascial canal Jugular foramen. Tensor tympani
- 14. Tensor tympani Jugular foramen. Fascial canal Tympanic membrane Corda tympani canal
- 15. Tendon for Tensor tympani Jugular foramen.Osseous fascial canal External auditory canal
- 16. Petrous Apex. Osseous fascial canal Inferior handle of malleus Jugular foramina. Jugular Bulb. Tendon for Tensor tympani
- 17. Tendon for Tensor tympani Apical turn of the cochlea Basal turn of the cochlea Handle of malleus Osseous fascial canal
- 18. Handle of malleus Long process of Incus Osseous fascial canal 3rd portion Tendon for Tensor tympani Cochlear process Basal turn of cochlea Aqueduct of cochlea Promontory
- 19. Head of malleus Wall for middle ear Body of Incus Osseous fascial canal (3rd portion) Tendon for Tensor tympani Cochlear process Round window Pyramidal eminence
- 20. Pyramidal eminence VestibuleOsseous fascial canal (3rd portion)
- 21. Ovale Window Osseous fascial canal (2nd portion)
- 22. Osseous fascial canal (1st portion) Mastoid antrum Extreme upper jugular foramen.
- 23. Internal acoustic meatus Mastoid antrum Aditus ad antrum
- 24. Aditus ad antrum Lateral semicircular canal
- 25. Mastoid antrum
- 26. Mastoid antrum Mastoid foramen Upper jugular foramen. Vestibular aqueduct
- 27. Mastoid foramens
- 28. Mastoid canal Superior semicircular canal. Posterior semicircular canal. jugular foramen.
- 29. Mastoid antrum Ear pinna Foramina for internal jugular vein
- 30. internal jugular vein foramen Mastoid antrum
- 31. Mastoid antrum Ear pinna internal jugular vein foramen
- 33. Aditus ad antrum Bony canal for Corda tympanum 3rd portion of osseous fascial canal. internal jugular vein foramen Pyramidal eminence
- 34. Lateral semicircular canal. 3rd portion of osseous fascial canal. Ear pinna internal jugular vein foramen Pyramidal eminence Jugular -facial foramen
- 35. Lateral semicircular canal. Superior semicircular canal. internal jugular vein foramen Pyramidal eminence 3rd portion of osseous fascial canal.
- 36. Lateral semicircular canal. Superior semicircular canal. internal jugular vein foramen
- 37. Superior semicircular canal. internal jugular vein foramen Cochlear aqueduct Round window. Septum epitympanum jugulare
- 39. Lateral semicircular canal. 2nd portion of osseous fascial canal. Ovale window. Ear drum Vestibule Malleous Epitympanum
- 40. Epitympanum Tegmen tympani Incus Drum spur External auditory meatus Tympanic membrane Superior semicircular canal. Internal acoustic meatus Promontory
- 41. Epitympanum Tegmen tympani Drum spur Tympanic membrane Handle of malleous Petrous apex. 1st portion of osseous fascial canal Basal turn of cochlea
- 42. Tympanic membrane Drum spur Tegmen tympani malleous 1st portion of osseous fascial canal Internal acoustic meatus
- 43. 1st portion of osseous fascial canal Cochlea 2nd portion of osseous fascial canal Malleous Head Neck Handle Tendon for Tensor tympani Septum epitympanum jugulare
- 45. Geniculate ganglia. Myotendinous junction of tensor tympani Carotid canal Apex of Cochlea Petrous apex
- 46. Geniculate ganglia. Muscle belly of tensor tympani Aditus antrum Petrous apex Carotid canal
- 47. Muscle belly of tensor tympani Petrous apex Carotid canal Aditus antrum
- 48. Head of malleous Body of incus
- 49. Spiral laminar bone with cochlear apex Cochlea (basal turn)
- 50. Pyramidal eminence Promontory Sinus tympani. 3rd portion of osseous fascial canal Cavernous Tympanicum
- 51. The internal auditory canal: - Has three parts: the internal acoustic meatus (medial opening), the canal (an average of 8 mm) and the fundus, of irregular shape (modulates the passage of the VII and VIII cranial nerves). - Nervous contents: the facial nerve (the largest in size) and the cochleo-vestibular nerve that divides into the cochlear nerve and the vestibular nerve which further divides itself into the superior (innervates the utricle and the ampulla of the superior and lateral SCC), and the inferior branches (innervates the saccule and the ampulla of the posterior SCC). The singular nerve (or the posterior ampullary nerve) has its proper canal, the singular canal, in the postero-inferior quadrant of the fundus that can be often be observed with 3T imaging. - Vascular content: arterial by the labyrinthine artery and venous with three drainage pathways (internal auditory vein, vein of cochlear aqueduct and vein of vestibular aqueduct). The inner ear MR anatomy.
- 55. Axial section through the inner auditory canal (IAC) and the labyrinthe with visualization of the cochlear and inferior vestibular nerves. The utricular macula is also well depicted.
- 56. Anterior coronal section through the IAC. Outline of the facial nerve in its complete cisternal course, the cochlear nerve is only partially viewed.
- 57. Posterior coronal section through the IAC. Vestibular nerve division and vestibular ganglion (of Scarpa) are visualized.
- 58. Appearance variant of the vestibular nerve with inferior vestibular division into the saccular nerve (that innerves the saccule) and the posterior ampullary nerve (for the ampulla of the posterior semicircular canal). The singular canal is also frequently observed, not shown in this figure. Coronal and sagittal sections through the IAC.
- 59. Sagittal seriate sections of the IAC from medial (left), showing the pontocerebellar cistern, to lateral (right), showing the fundus and inner ear structures.
- 60. Cochlear nerve at the fundus of the IAC and its passage via the modiolus to the cochlea in an oblique sagittal section. This finding is of clinical importance when studying the inner ear malformations.
- 61. Heavily T2 coronal section respective to the IAC. Vestibular and cochlear structures are seen, note the utricular macula and spiral lamina.
- 62. Sagittal section respective to the IAC through the inner ear in a 3D Heavily T2 sequence. This section is also orthogonal to the macula of the utricle and unfolds partially the cochlea.
- 63. Oblique coronal section through the anterior labyrinth and fundus of the IAC, 3D Heavily T2 sequence.
- 64. FLAIR sequence in the axial plane four hours after Gd intravenous injection, the saccule and part of the utricle are visualized.
- 65. Axial FLAIR Gd sequence through the utricle, the saccule is partially visualized.
- 66. Heavily T2 in the plane of the lateral semicircular canal (oblique axial). The ampulla and its ampullary crest (low signal) are seen.
- 67. FLAIR Gd sequence section in the lateral SCC plane, passing through the utricle.
- 68. Section in the plane of the superior semicircular canal (plane of Pöschl, sagittal to the petrous bone), with heavily T2 sequence.
- 69. Section in the same plane of the superior semicircular canal with FLAIR Gd sequence.
- 70. T2 sequence in the plane of the posterior SCC (plane of Stenver, coronal to the petrous bone). Notice the common part of the superior and posterior semicircular canals, i.e. the common crus.
- 71. FLAIR and Heavily T2 sequences, sections in the coronal plane. Notice the position of the utricular macula (T2 sequence) relative to the utricle (FLAIR).
- 72. Thank You.