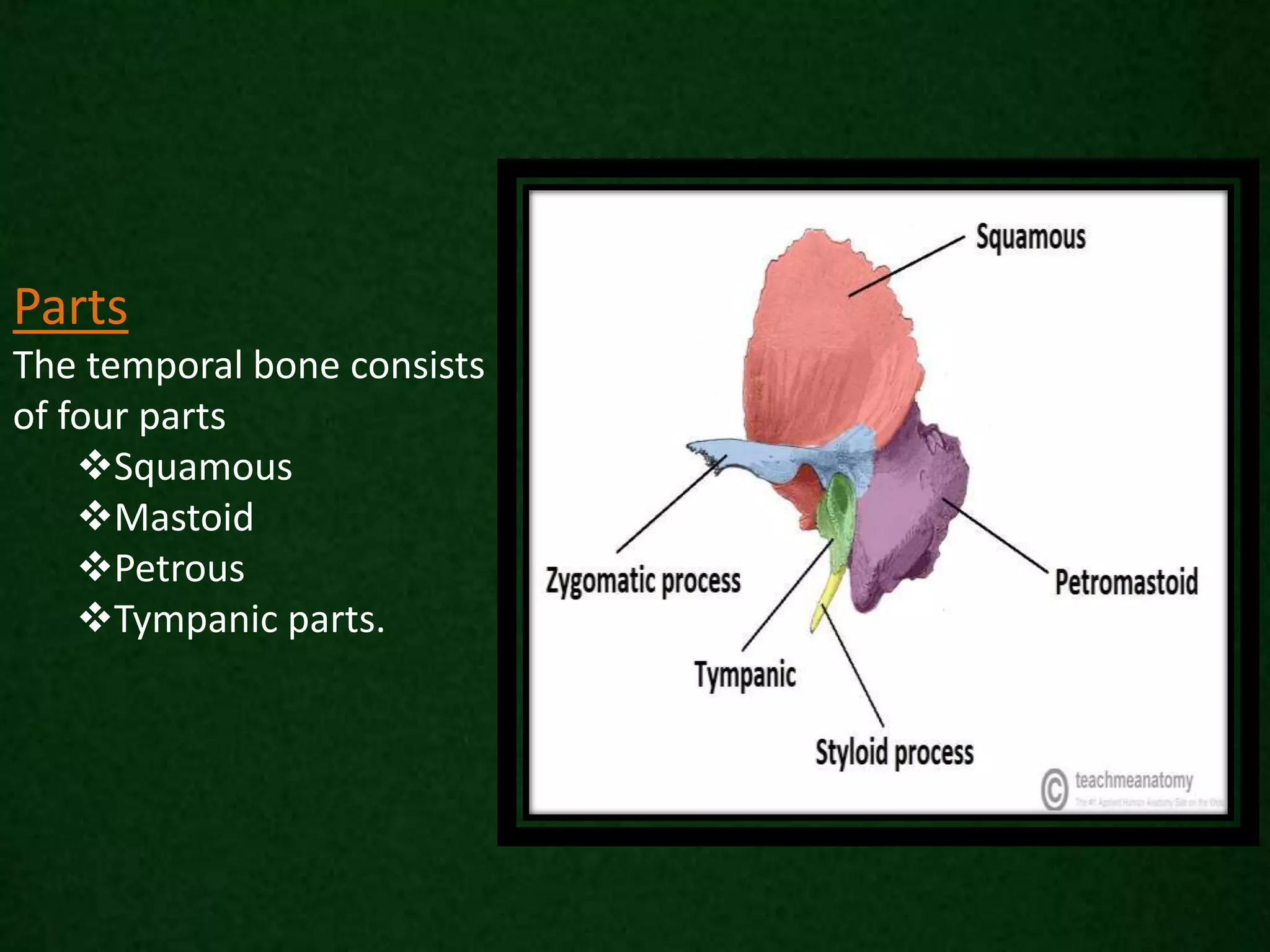
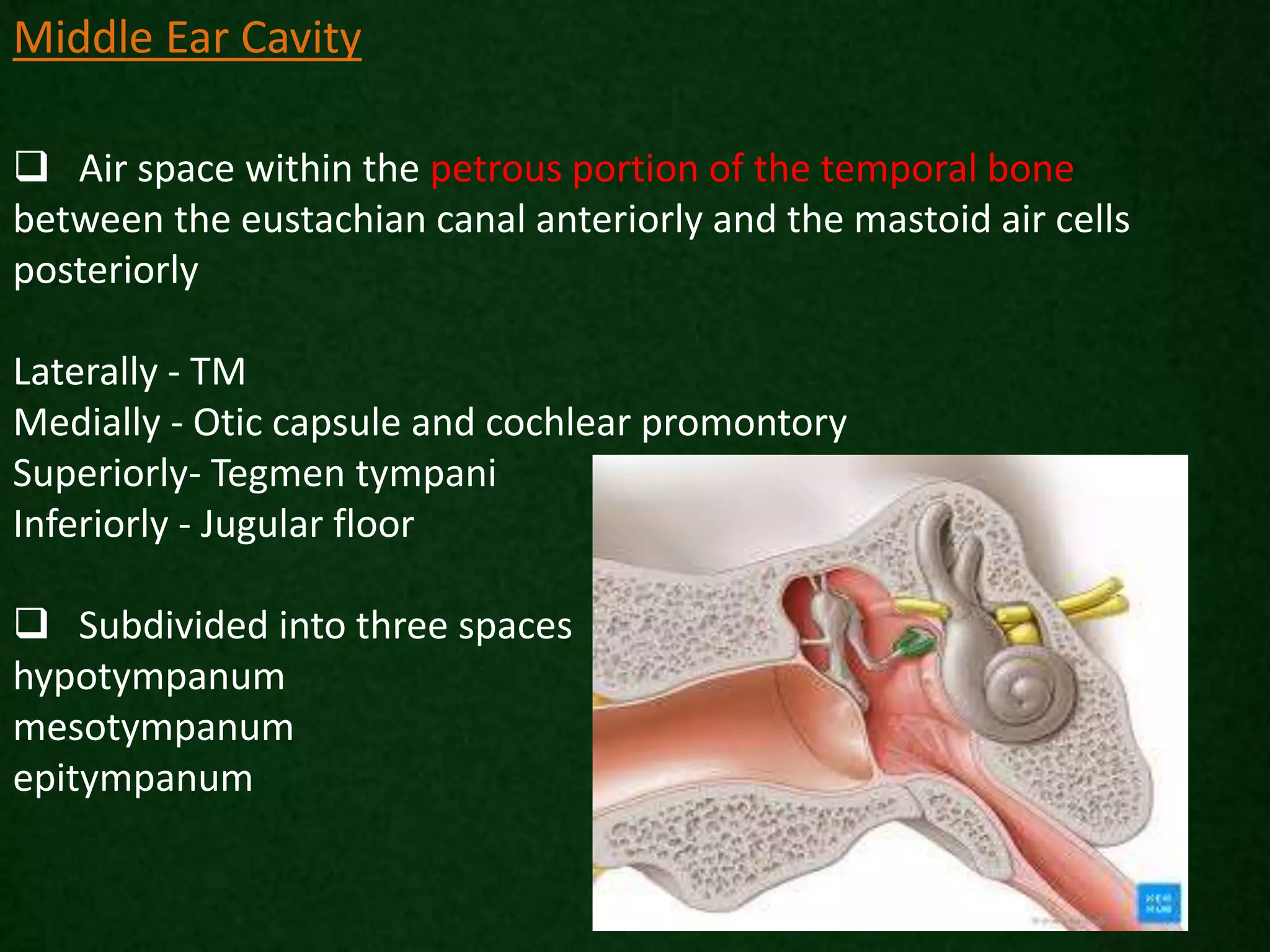
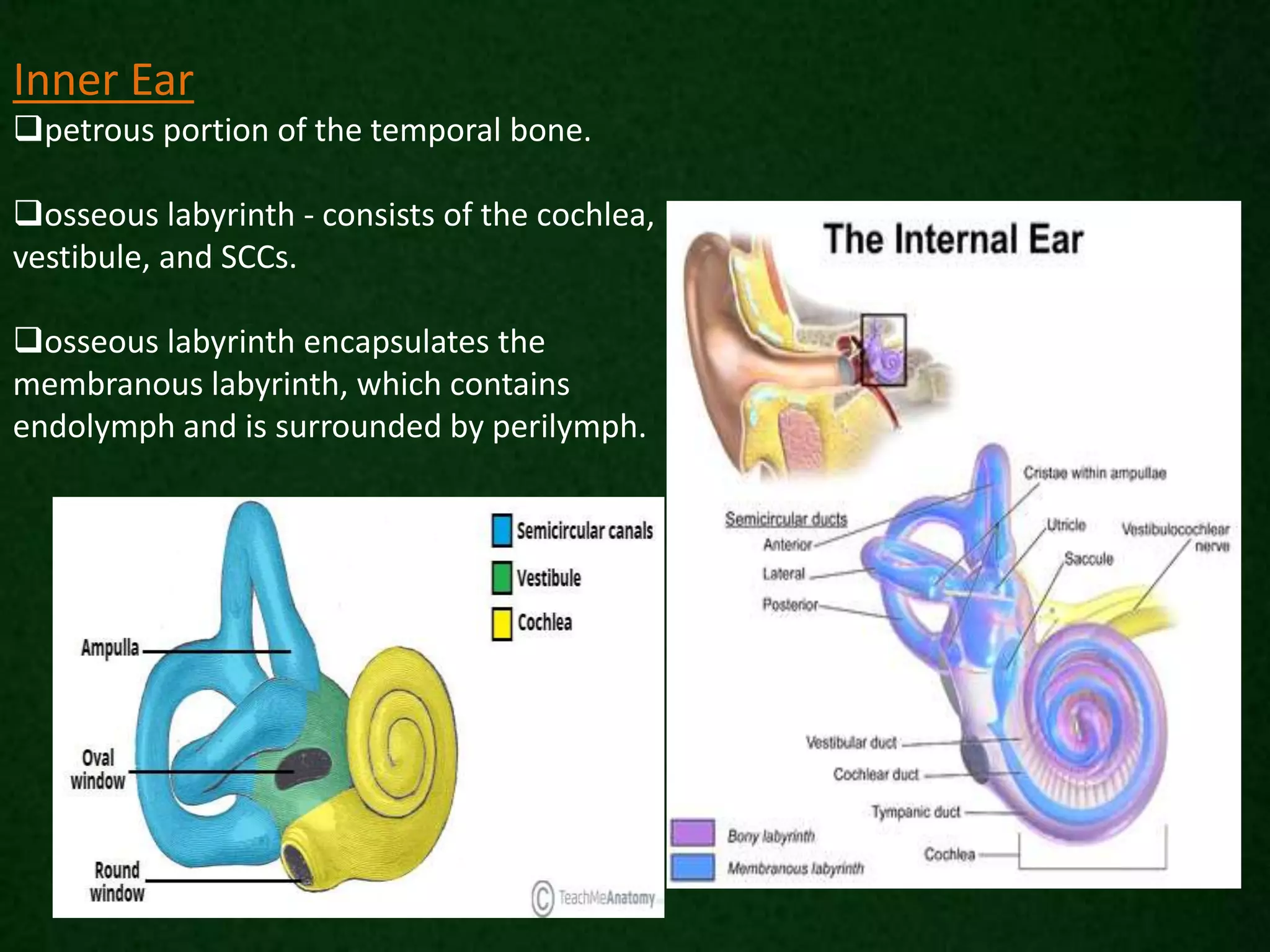
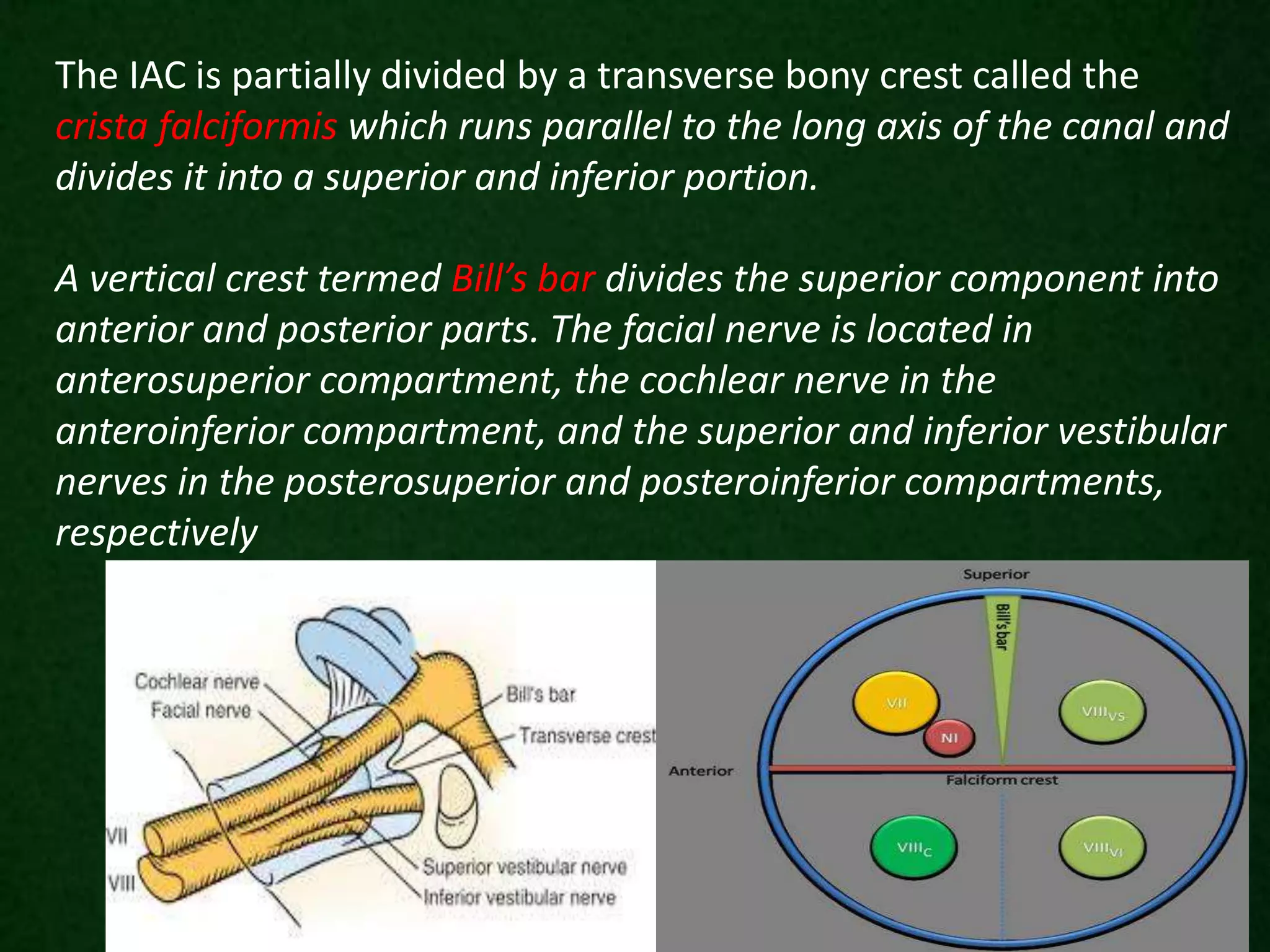
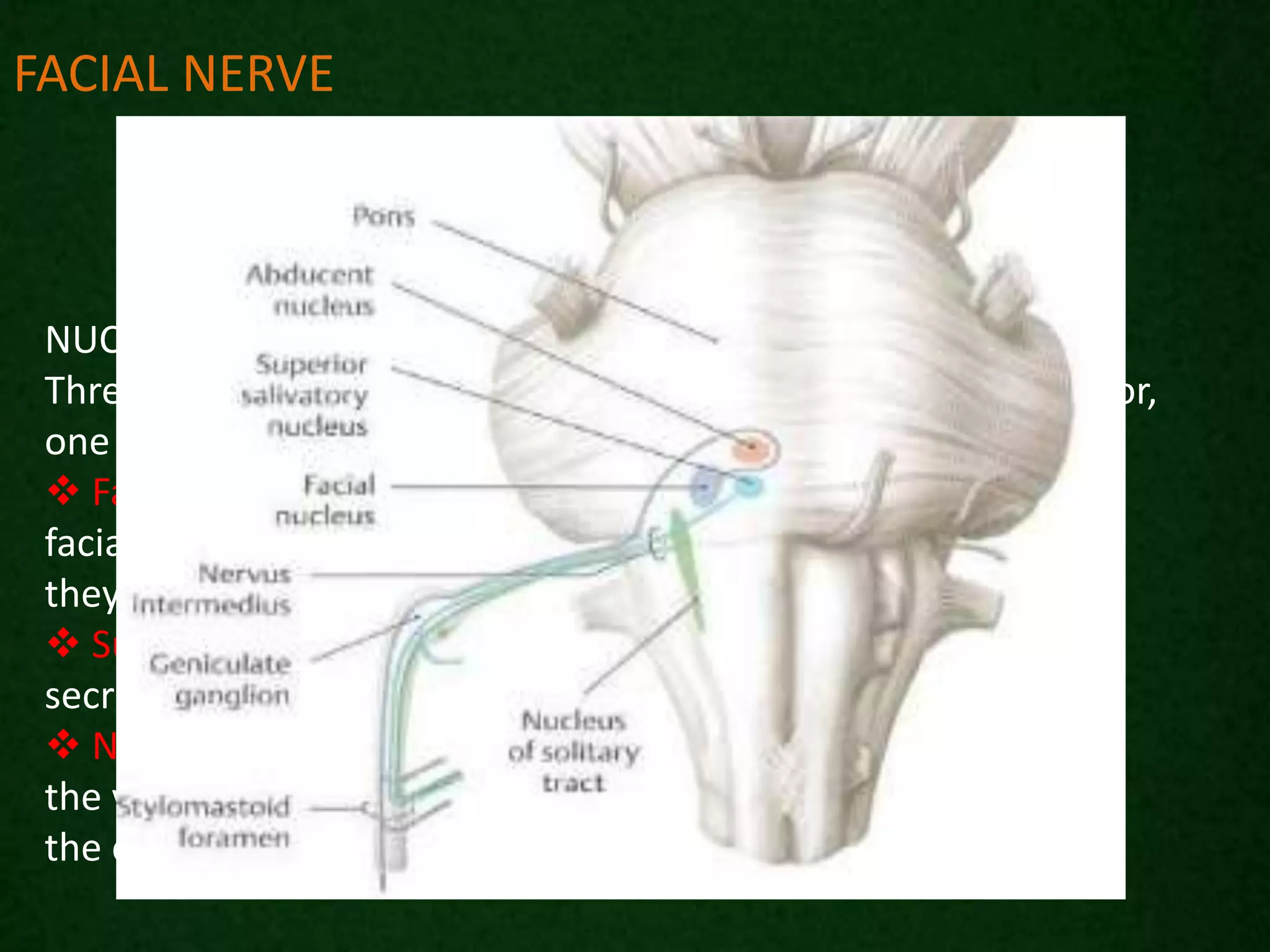
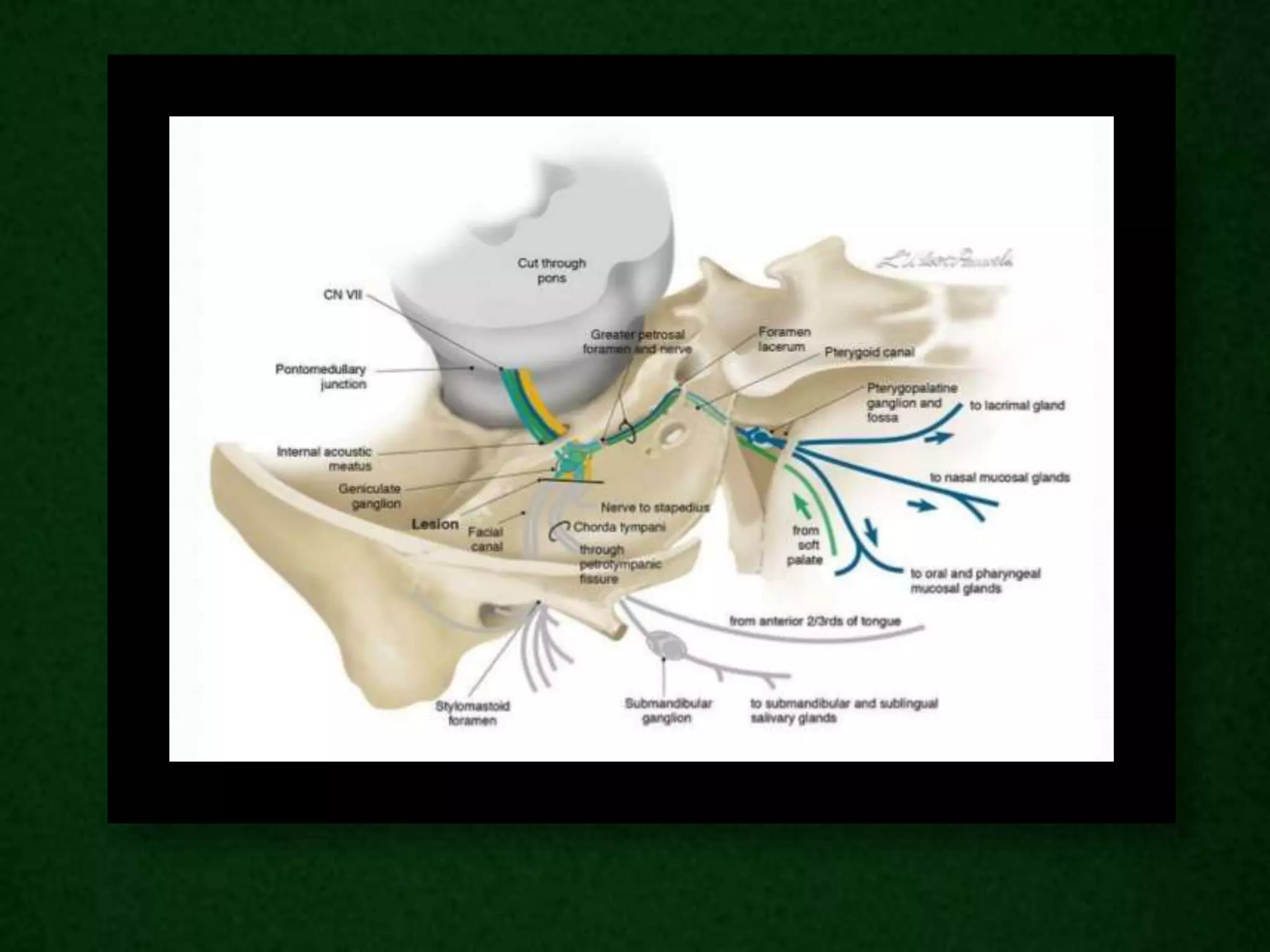
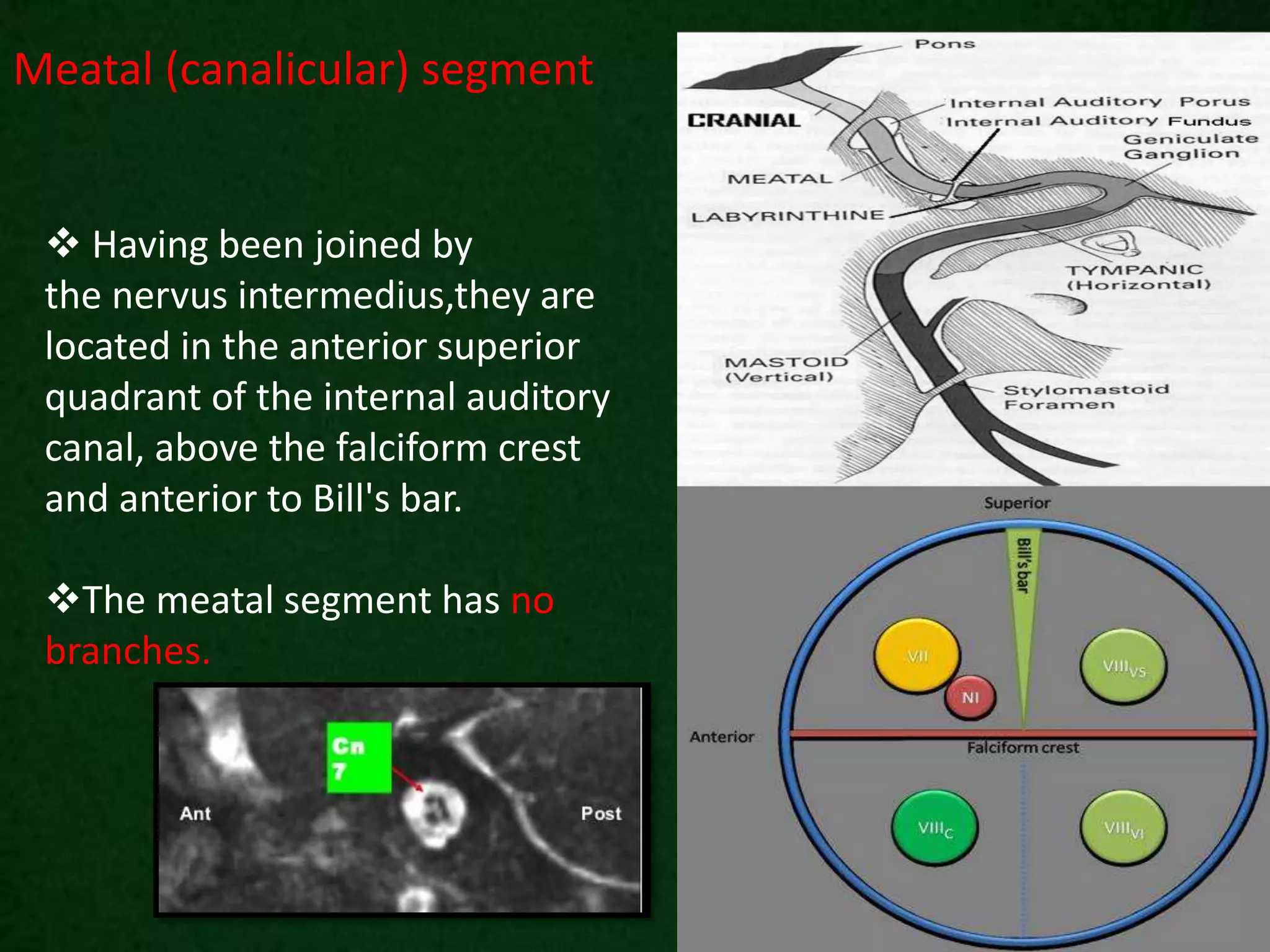
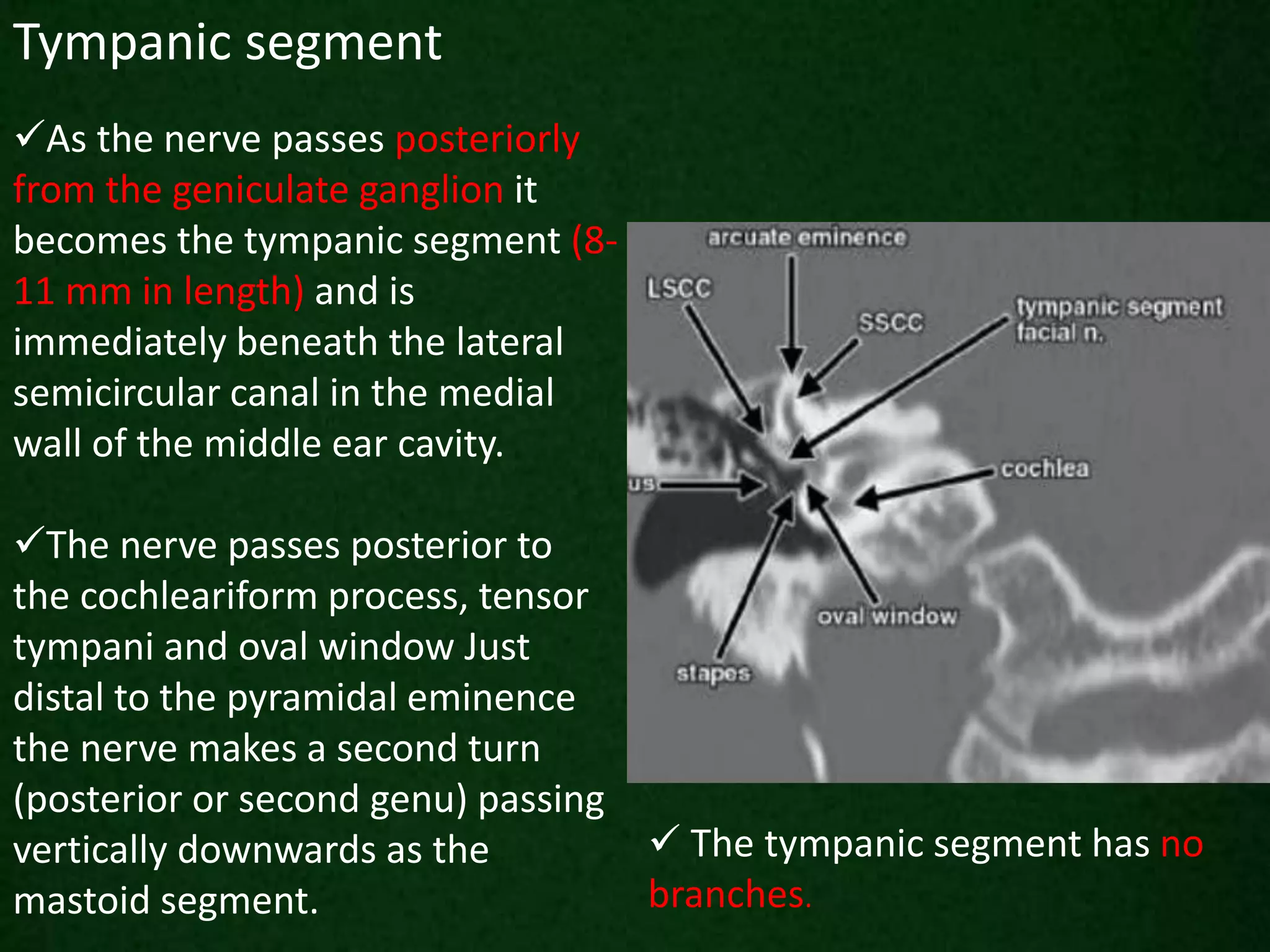
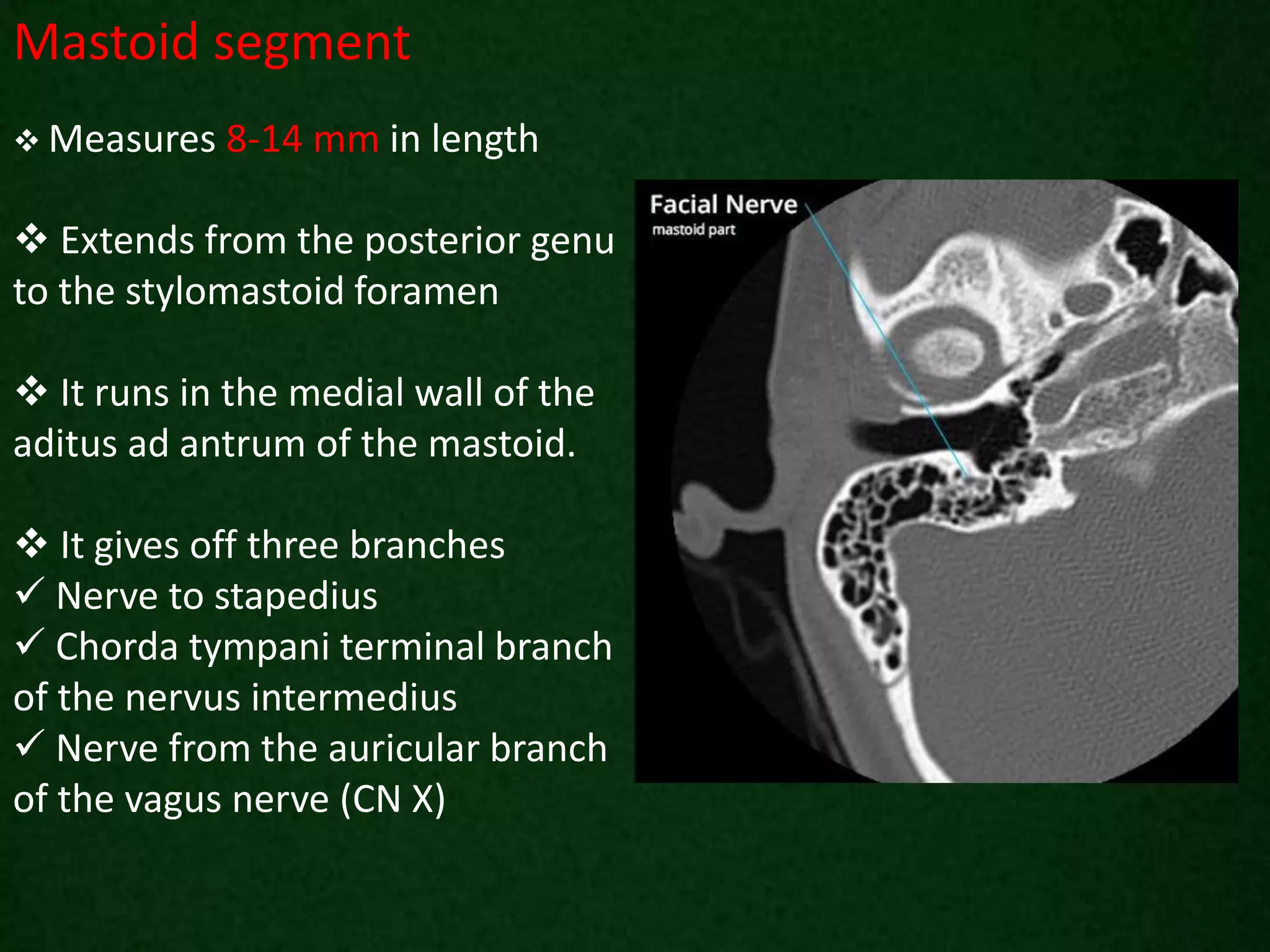
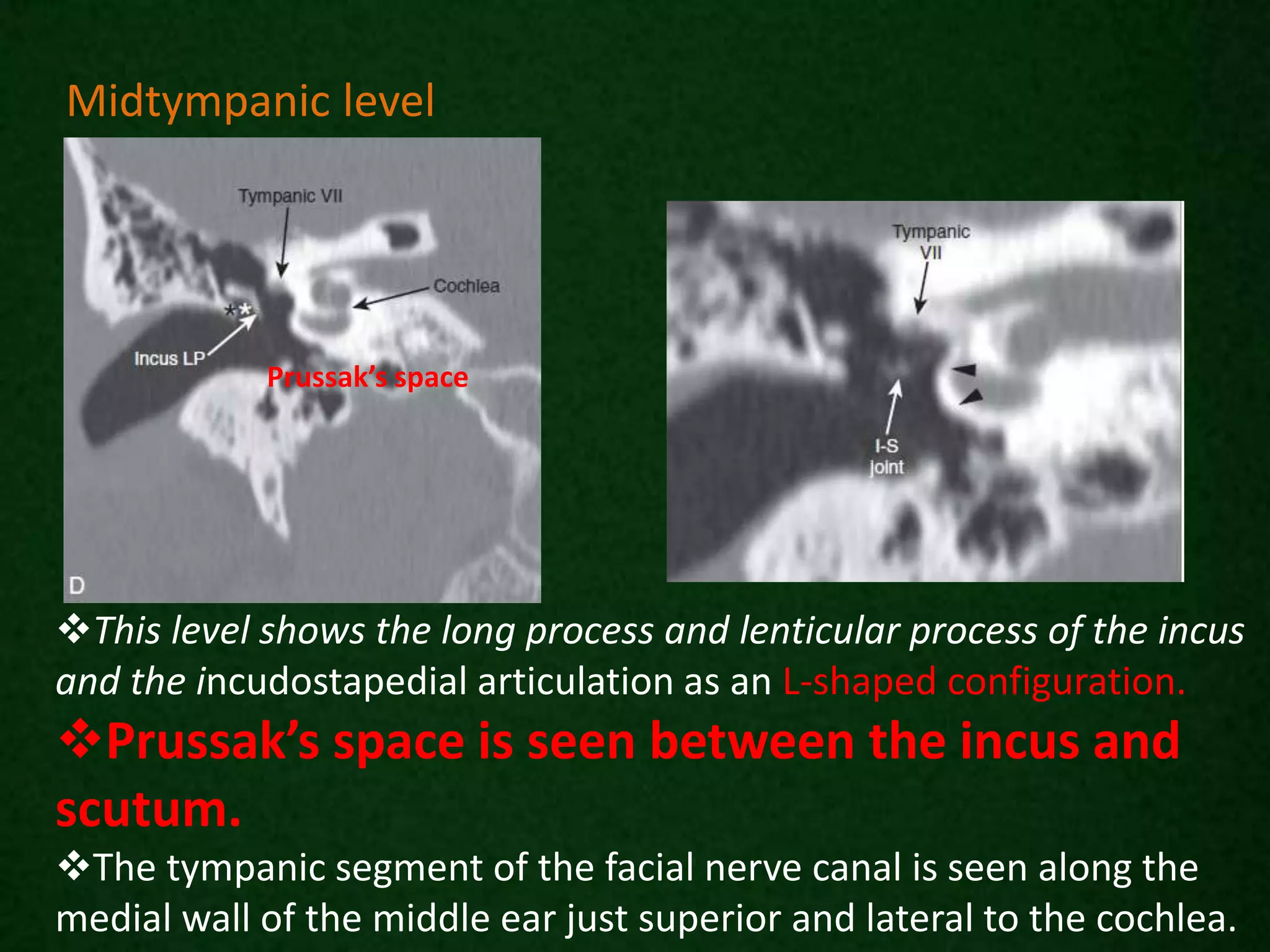
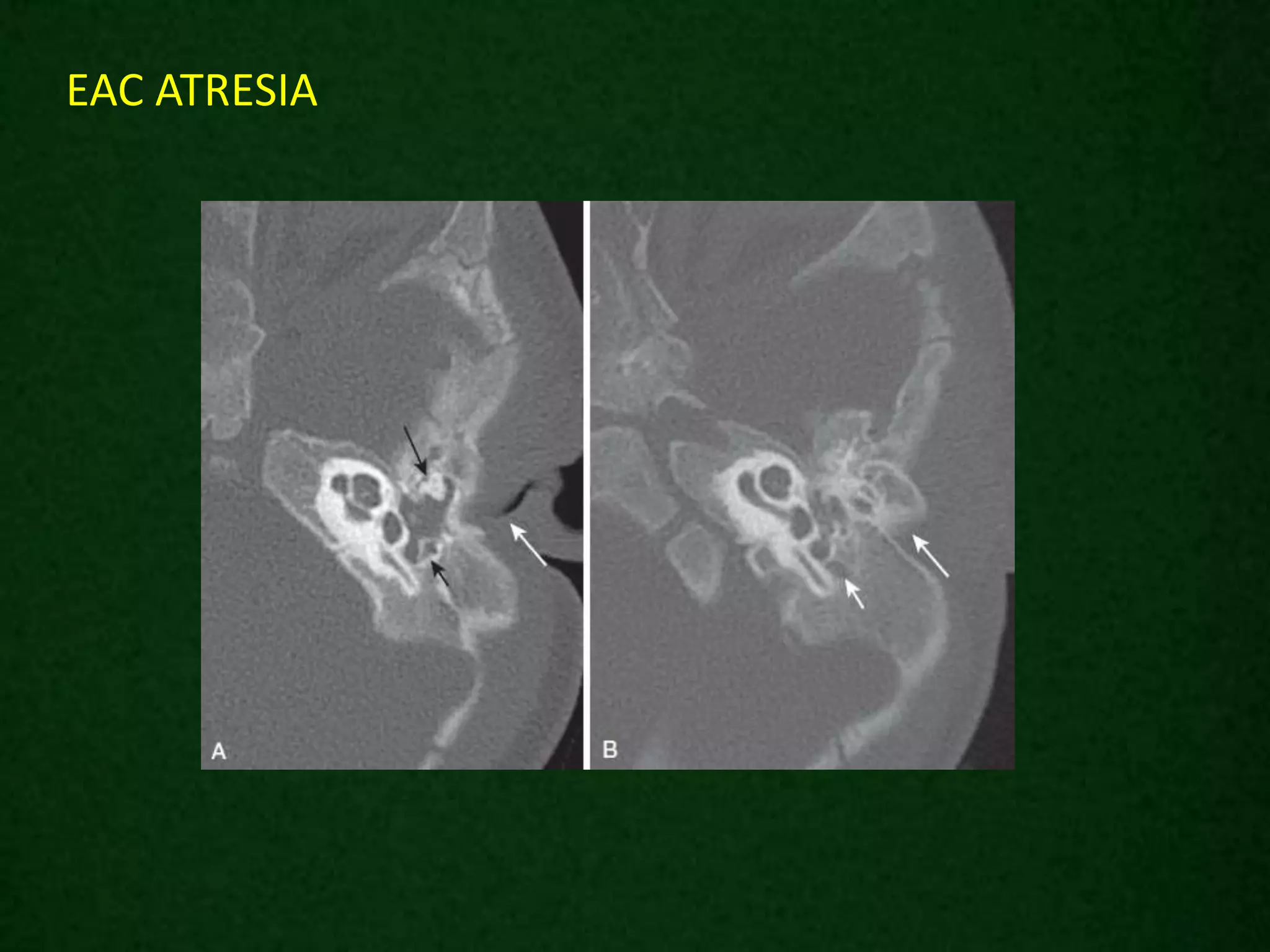
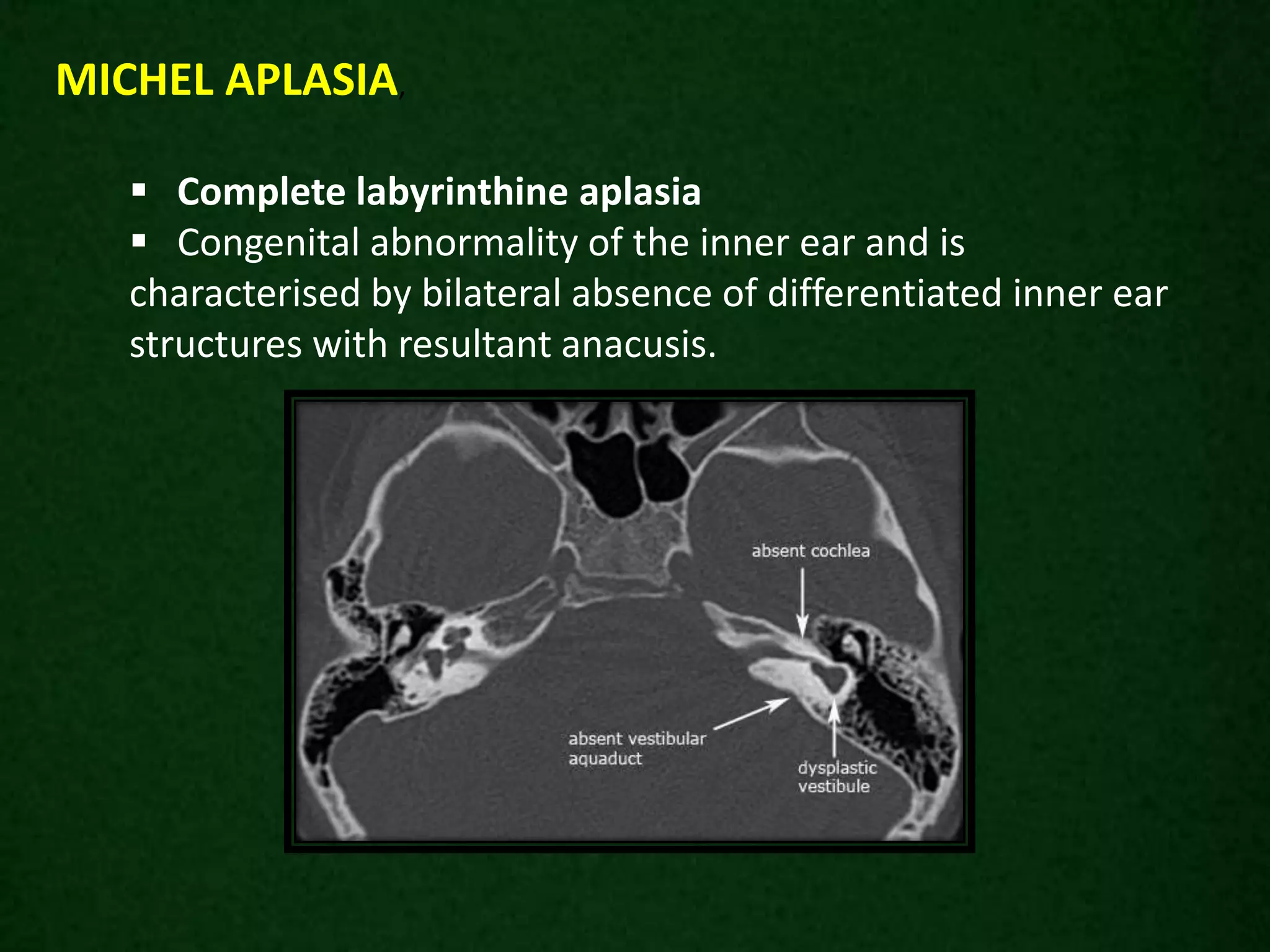
The document describes the anatomical structures of the temporal bone, including its four parts - squamous, mastoid, petrous, and tympanic. It details the locations and structures of the mastoid process, styloid process, zygomatic process, external acoustic meatus, middle ear cavity, mastoid antrum, ossicles, inner ear, internal auditory canal, carotid canal, jugular foramen and fossa, and course of the facial nerve. CT and MRI are described as the main imaging techniques used to evaluate the temporal bone, with CT excellent for osseous structures and MRI better for soft tissues.





























































































![Spleen[1]](https://cdn.slidesharecdn.com/ss_thumbnails/spleen1-171112094140-thumbnail.jpg?width=640&height=640&fit=bounds)
![Stomach and duodenum_-_benign_lesions[2]](https://cdn.slidesharecdn.com/ss_thumbnails/stomachandduodenum-benignlesions2-171112093735-thumbnail.jpg?width=640&height=640&fit=bounds)

![Radiological anatomy of_abdomen[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyofabdomen1-170830125353-thumbnail.jpg?width=640&height=640&fit=bounds)



















