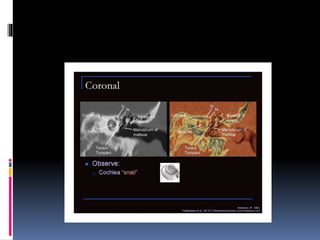
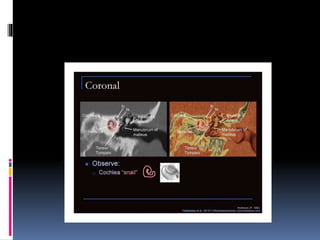
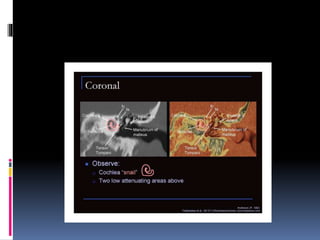
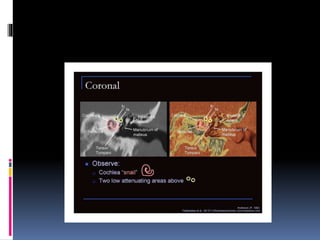
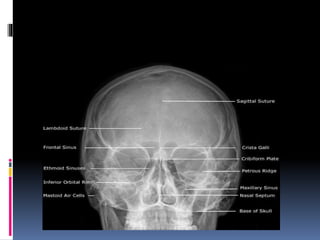
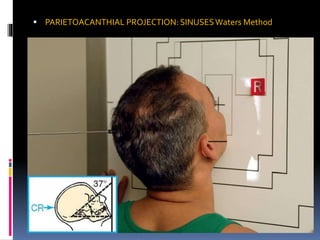
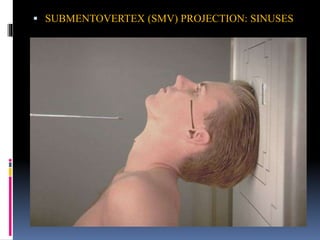
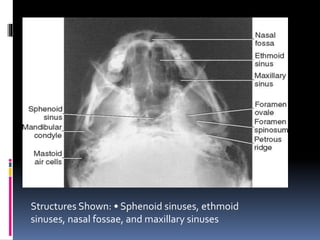
This document provides an overview of imaging modalities used in evaluating the ear, nose, and paranasal sinuses. It discusses plain radiography views including lateral, Caldwell, Waters, and submentovertex views. CT imaging of the nose and paranasal sinuses is described as the gold standard, with details on interpreting coronal and axial cuts. Key anatomical structures like the frontal sinus, ethmoid air cells, and sphenoid sinus are identified on various imaging views.






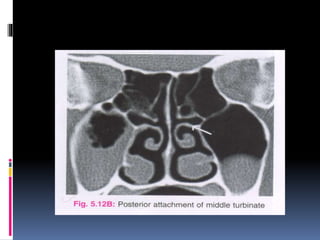














































![Radiography of skull [Autosaved].pptxriuyowioehgg](https://cdn.slidesharecdn.com/ss_thumbnails/radiographyofskullautosaved-251211014507-1d75cfe3-thumbnail.jpg?width=640&height=640&fit=bounds)



























