Downloaded 12 times

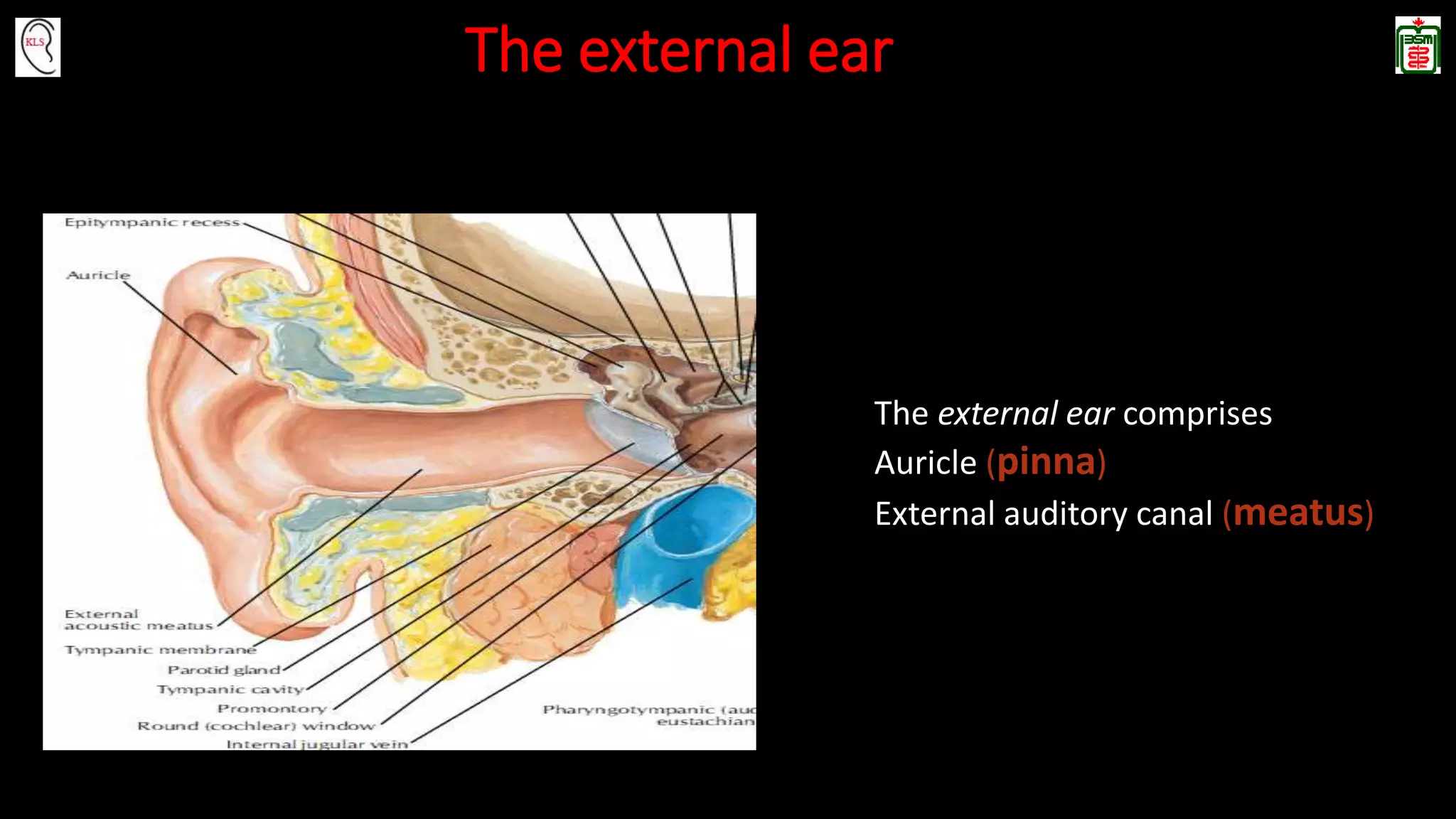


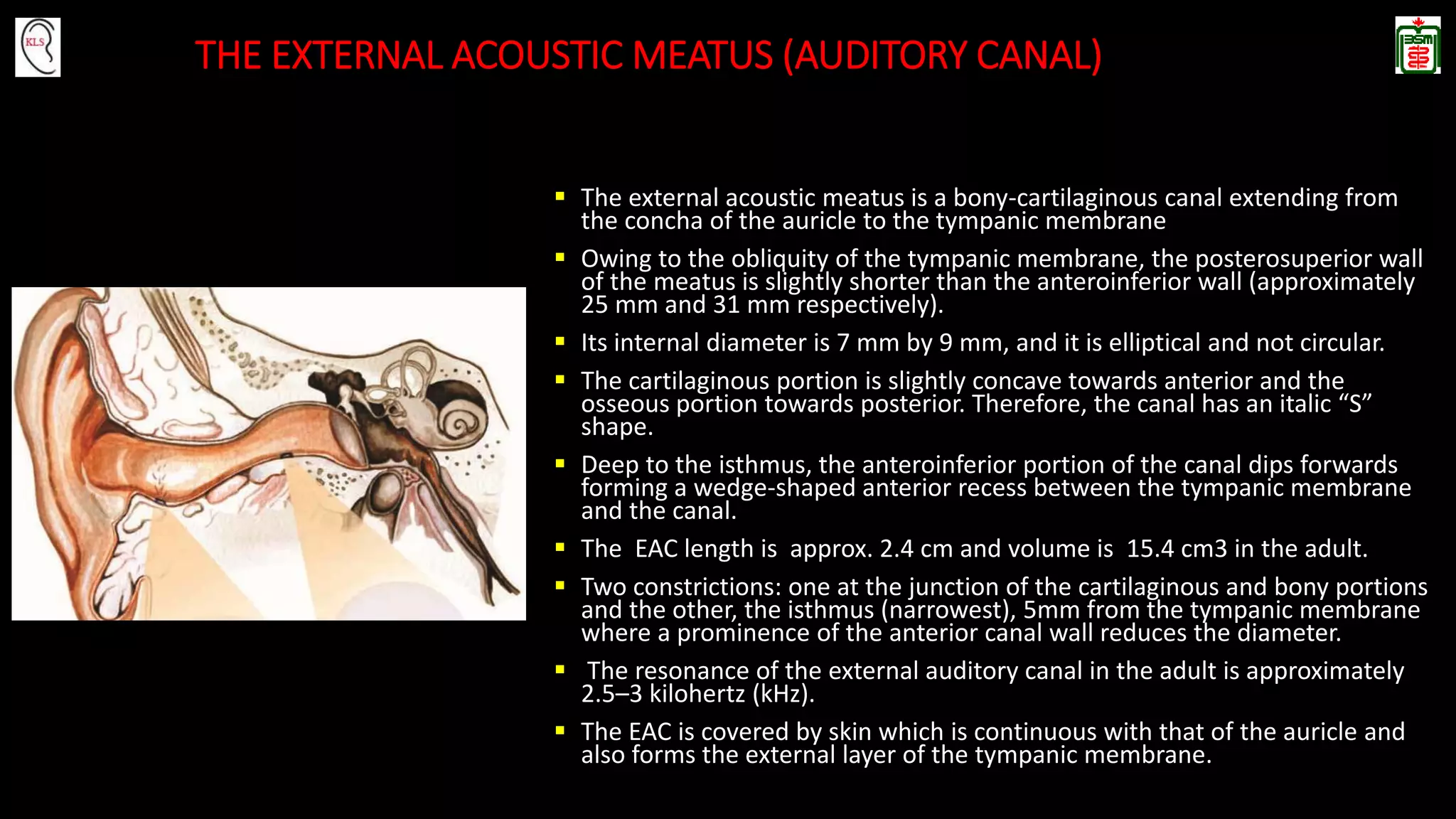

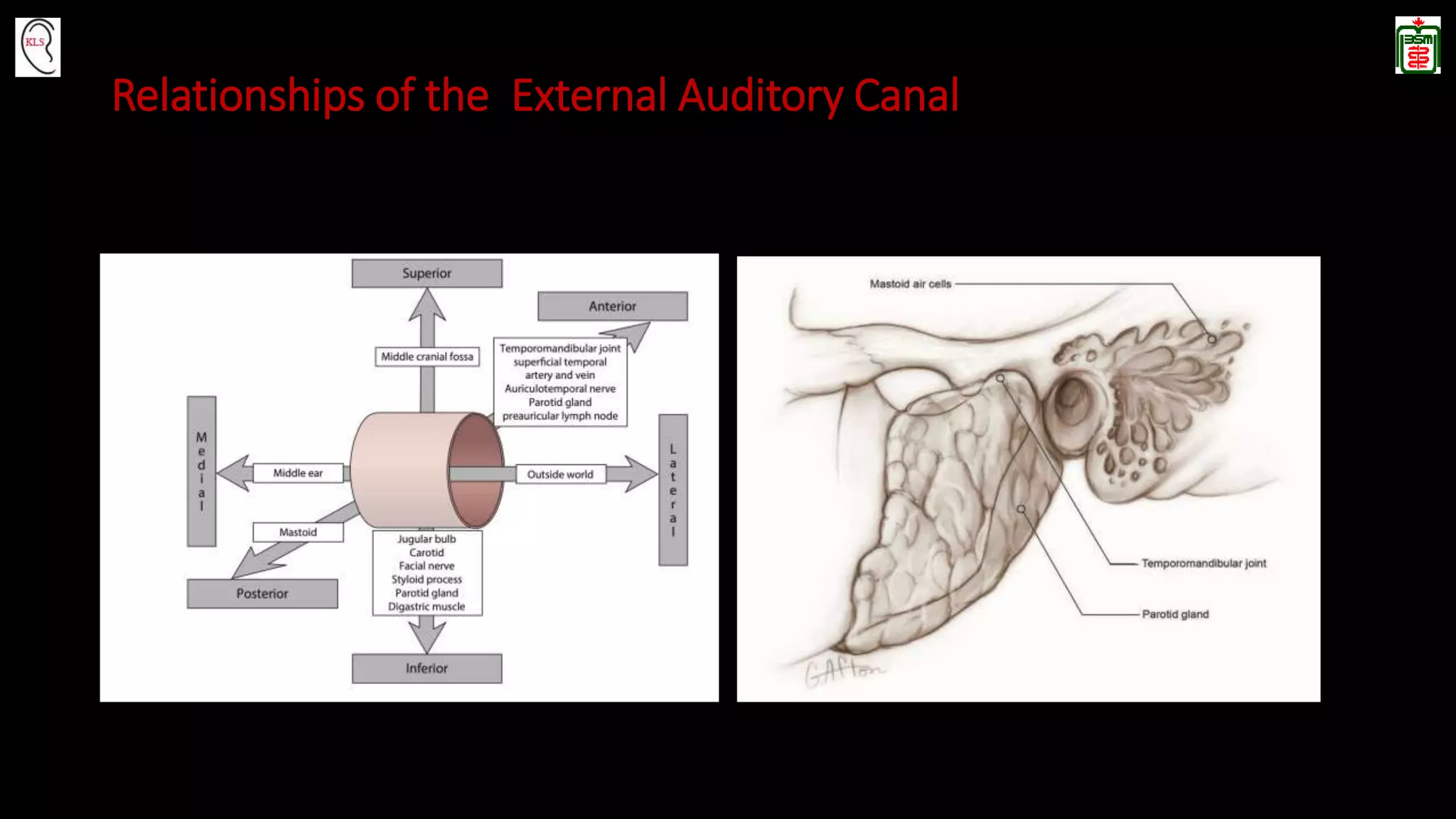


The external auditory canal is a bony-cartilaginous canal that extends from the auricle to the tympanic membrane. It has both cartilaginous and bony segments, with the cartilaginous segment forming the lateral one-third and the bony segment forming the medial two-thirds. The skin of the canal contains glands and hair follicles. The canal receives its blood supply from branches of the external carotid artery and its nerve supply from the trigeminal, facial, and vagus nerves. It has an average length of 2.4 cm and guides sound waves from the external environment to the tympanic membrane.