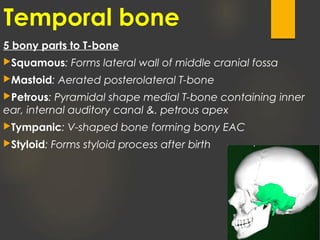
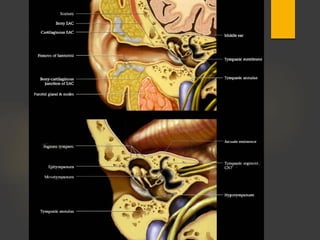
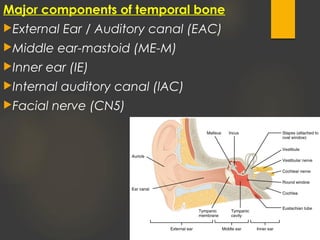
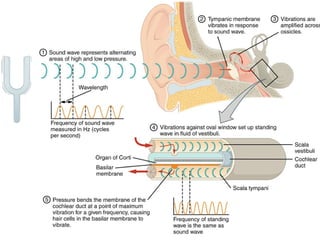
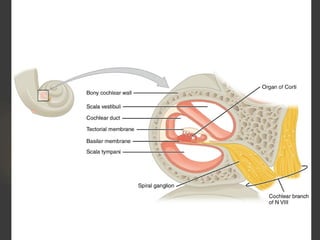
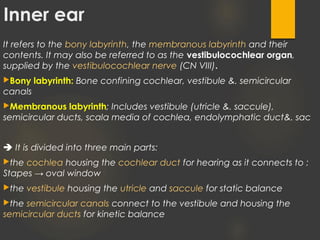
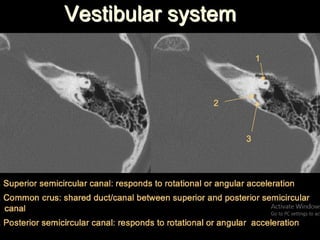
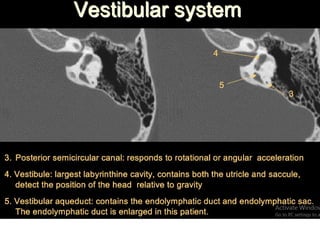
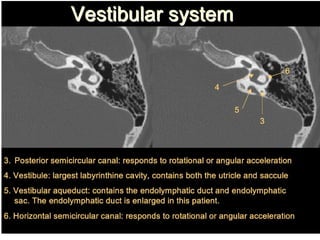
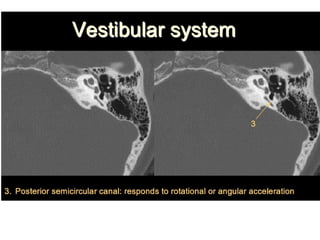
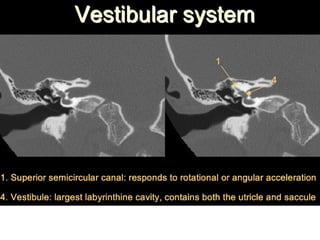
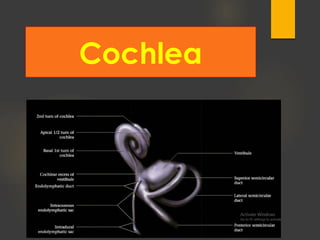
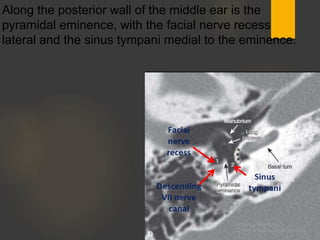
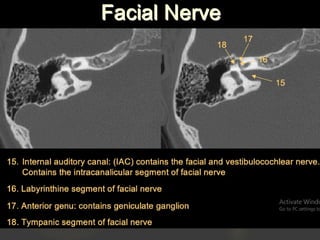
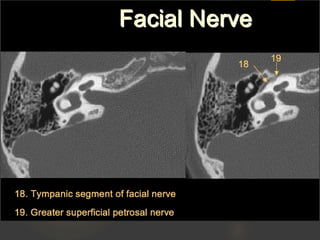
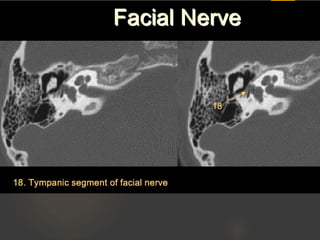
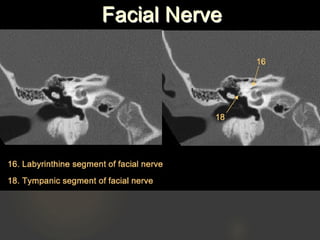
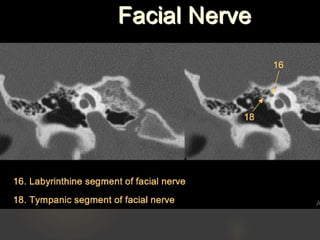
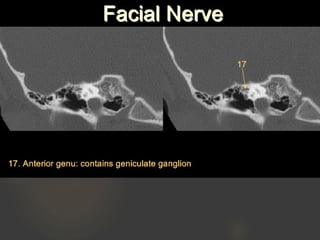
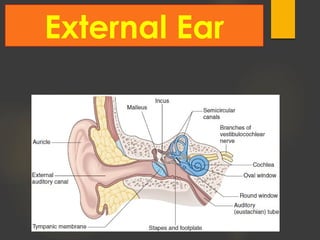
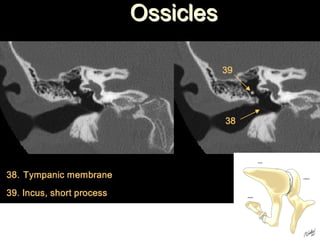
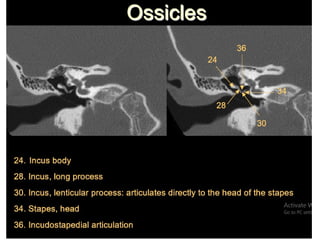
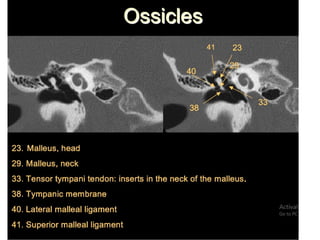
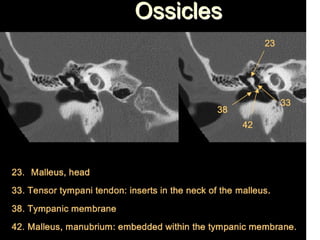
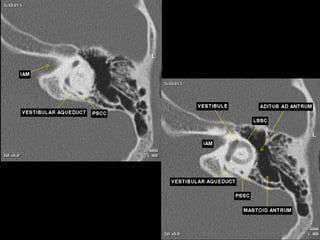
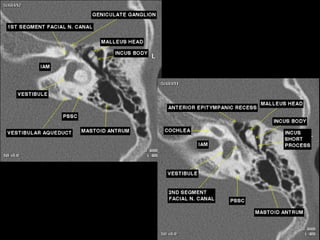
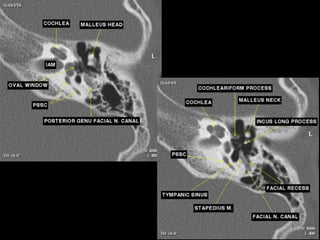
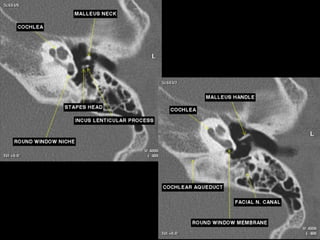
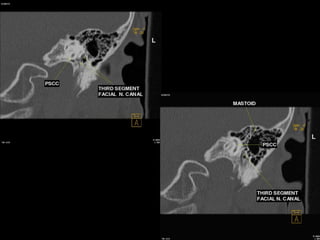
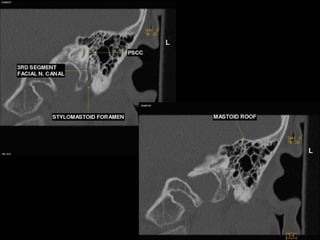
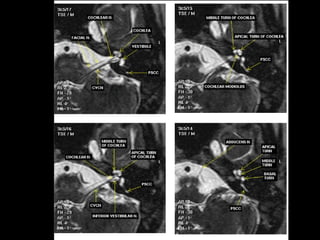
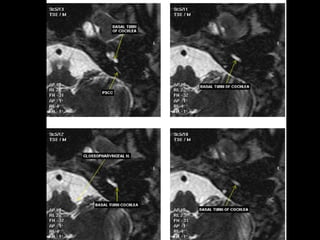
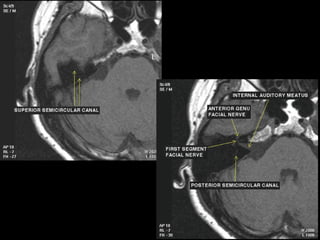
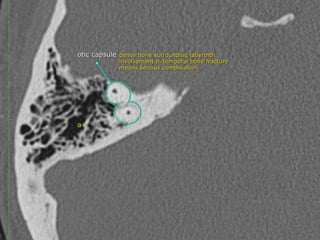
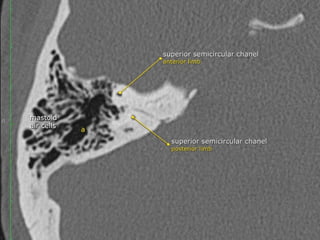
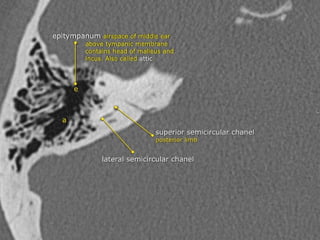
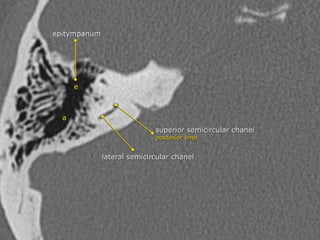
The document provides an overview of temporal bone anatomy, focusing on the petrous bone and inner ear structures. It describes the five parts of the temporal bone and how sound travels through the external ear canal to the oval window. Imaging techniques for evaluating the temporal bone such as CT and MRI are discussed. Key structures of the inner ear including the cochlea, vestibule, semicircular canals and their functions are explained in detail.


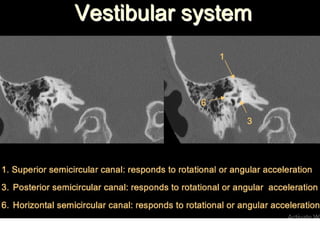
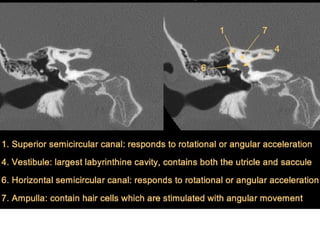














![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)






























































