Download as PPSX, PPTX
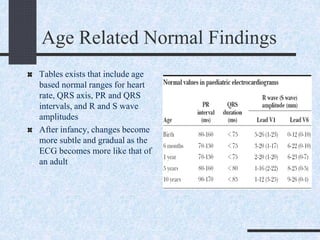
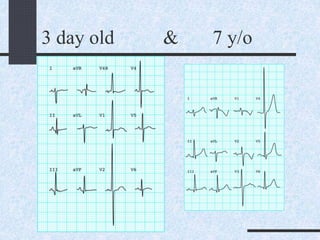
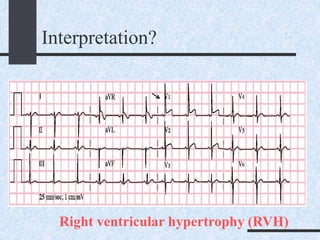
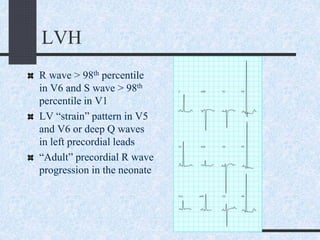
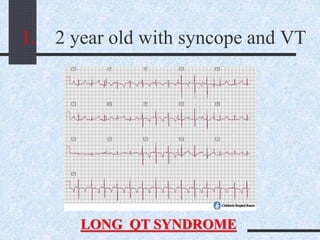
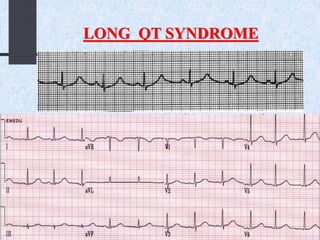
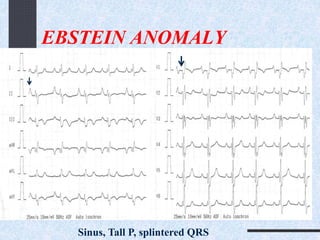
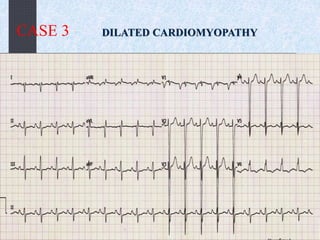
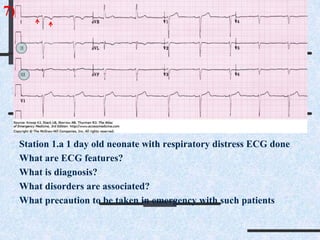

The ECG shows a pattern of right ventricular hypertrophy with a large R wave in lead V1 and deep S wave in lead V6, suggesting enlarged right ventricle. This, along with the juvenile T wave pattern of inverted T waves in the precordial leads from birth to age 8, are consistent with the normal developmental changes described in the document as the left ventricle increases in dominance from birth through childhood. The document provides an overview of normal pediatric ECG patterns and intervals across age groups as well as common arrhythmias and abnormalities.























































































