This document provides an overview of ECG interpretation including:
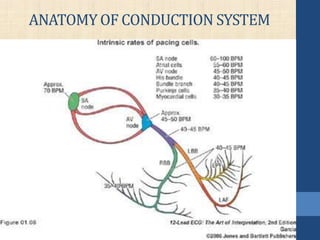
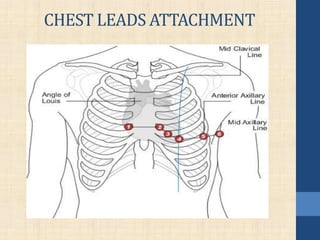
- The anatomy of the heart's conduction system and how ECG leads are attached
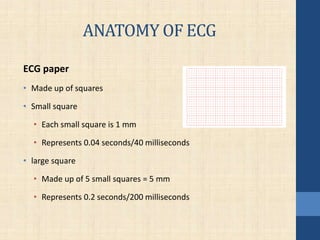
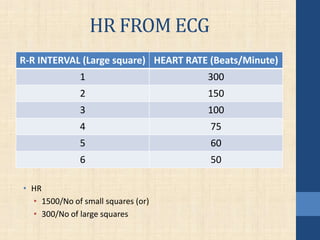
- How to read an ECG strip and calculate heart rate
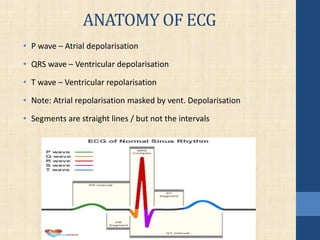
- Normal P, QRS, and T waves along with intervals like PR and QT
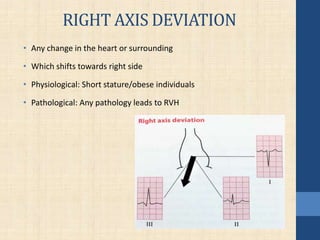
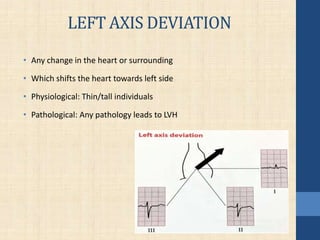
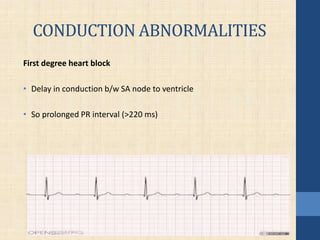
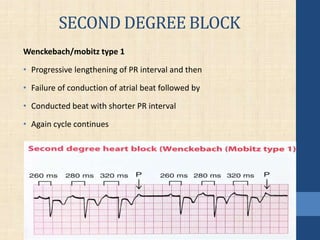
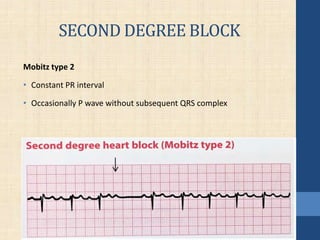
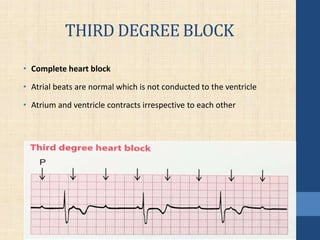
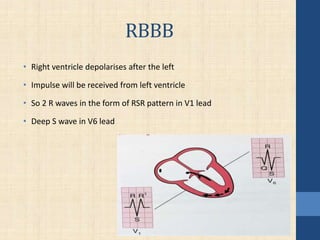
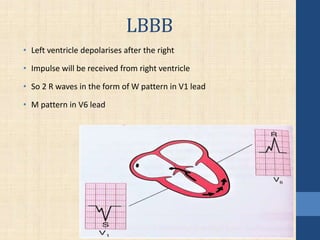
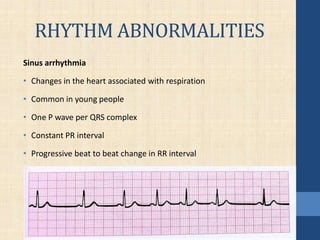
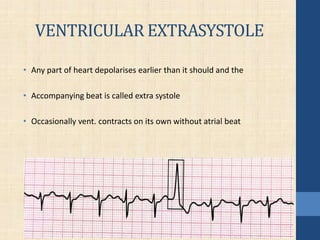
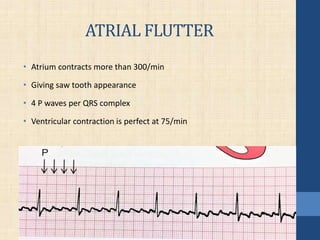
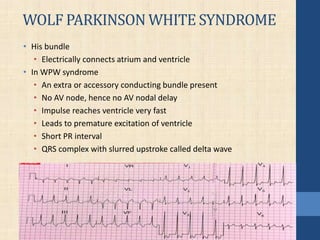
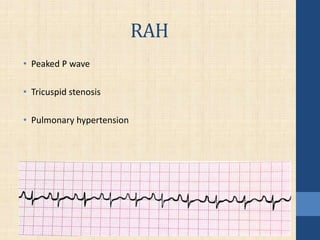
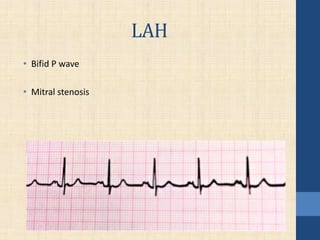
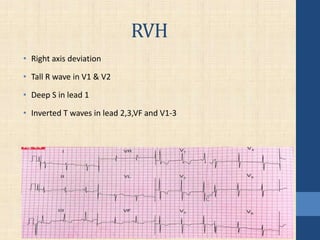
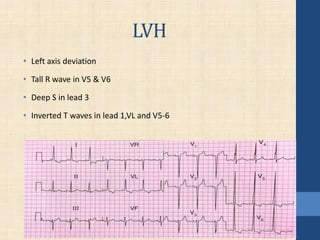
- Abnormalities that can indicate conditions like blocks, arrhythmias, and hypertrophy
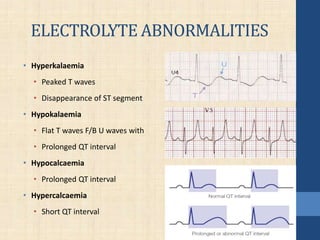
- Electrolyte imbalances that can affect the ECG tracing
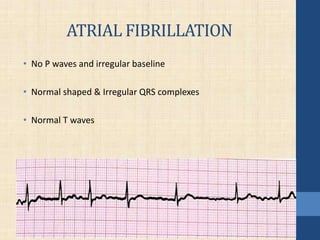
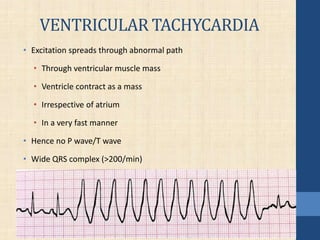
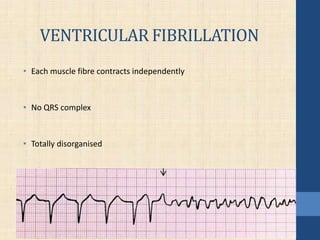
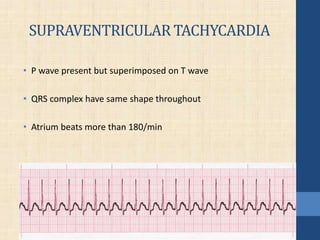
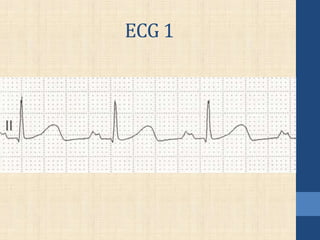
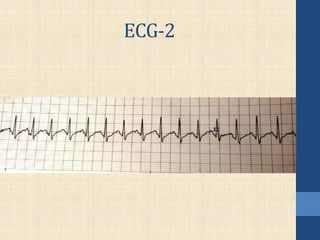
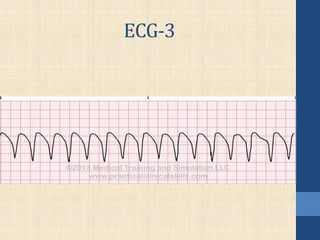
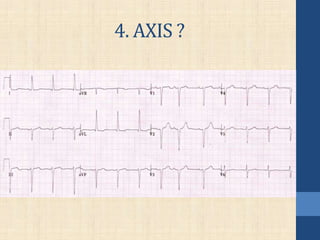
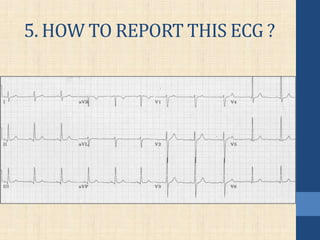
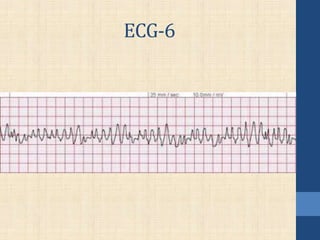
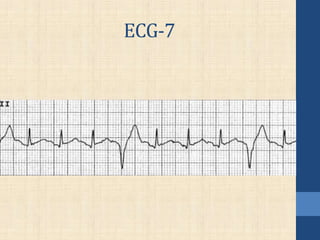
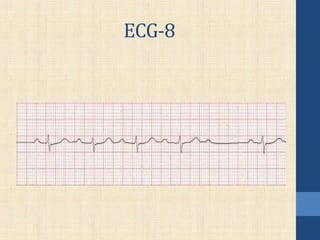
It concludes with examples of ECG strips and questions to test the reader's understanding.