Downloaded 97 times




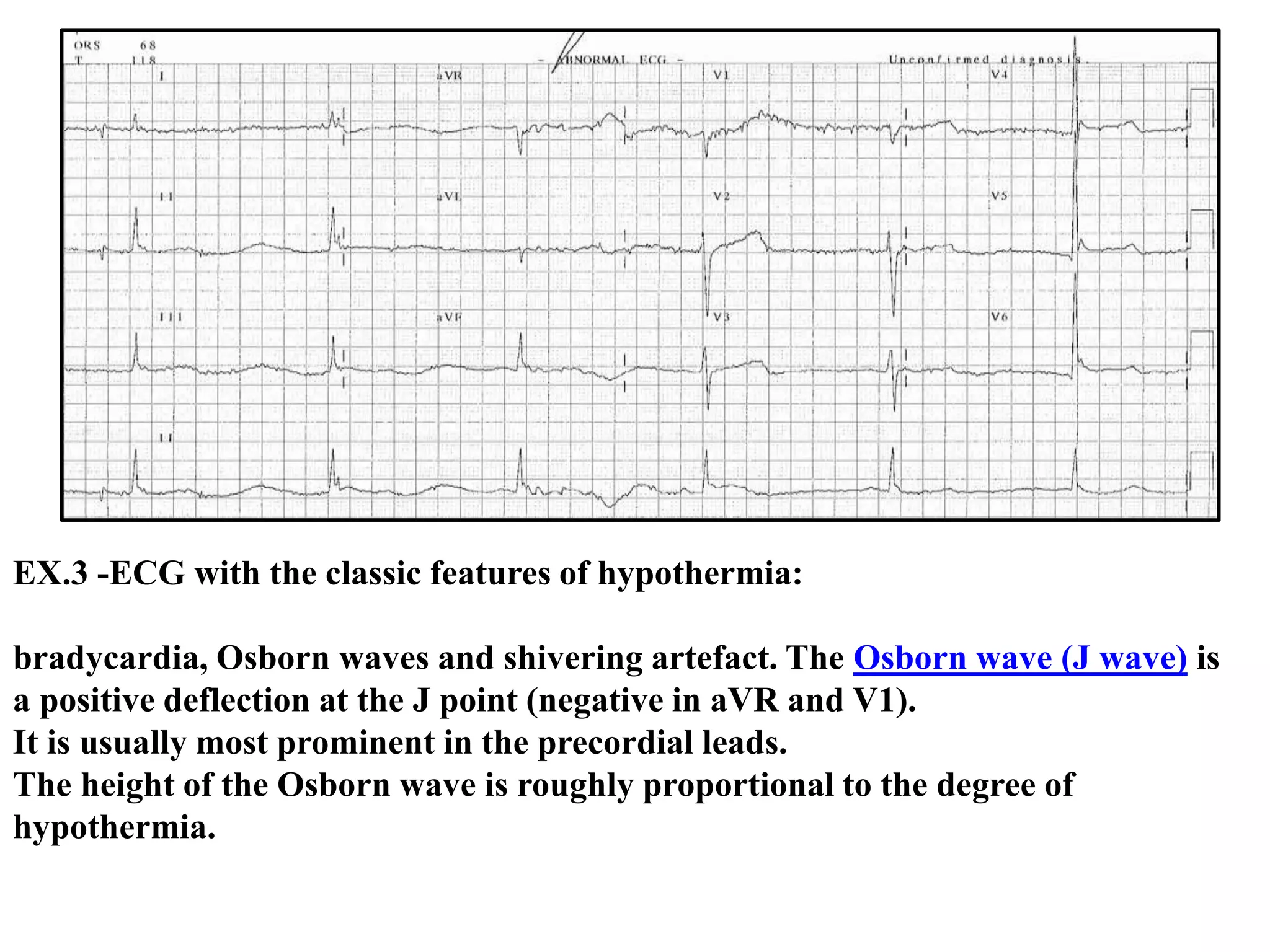













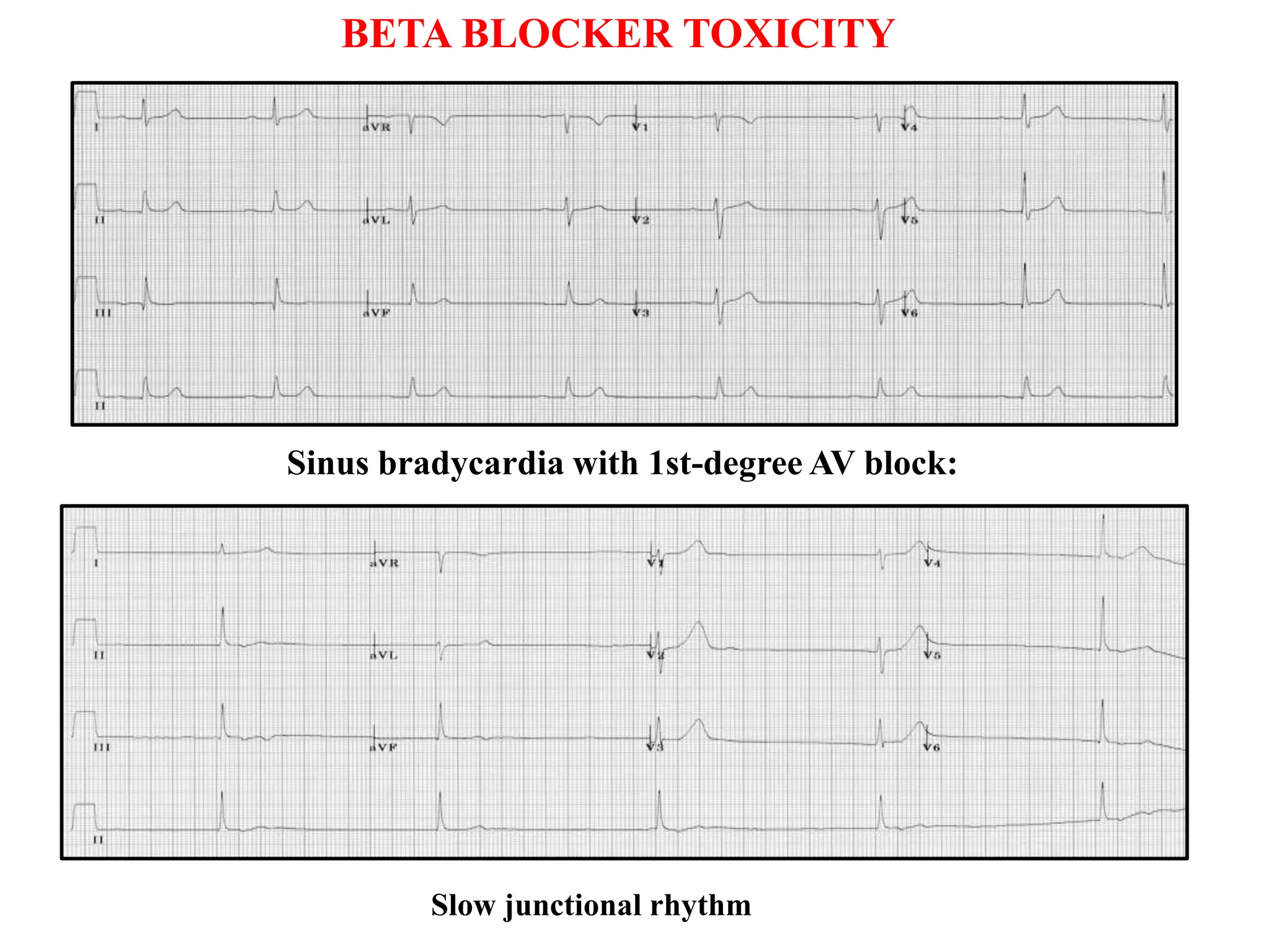





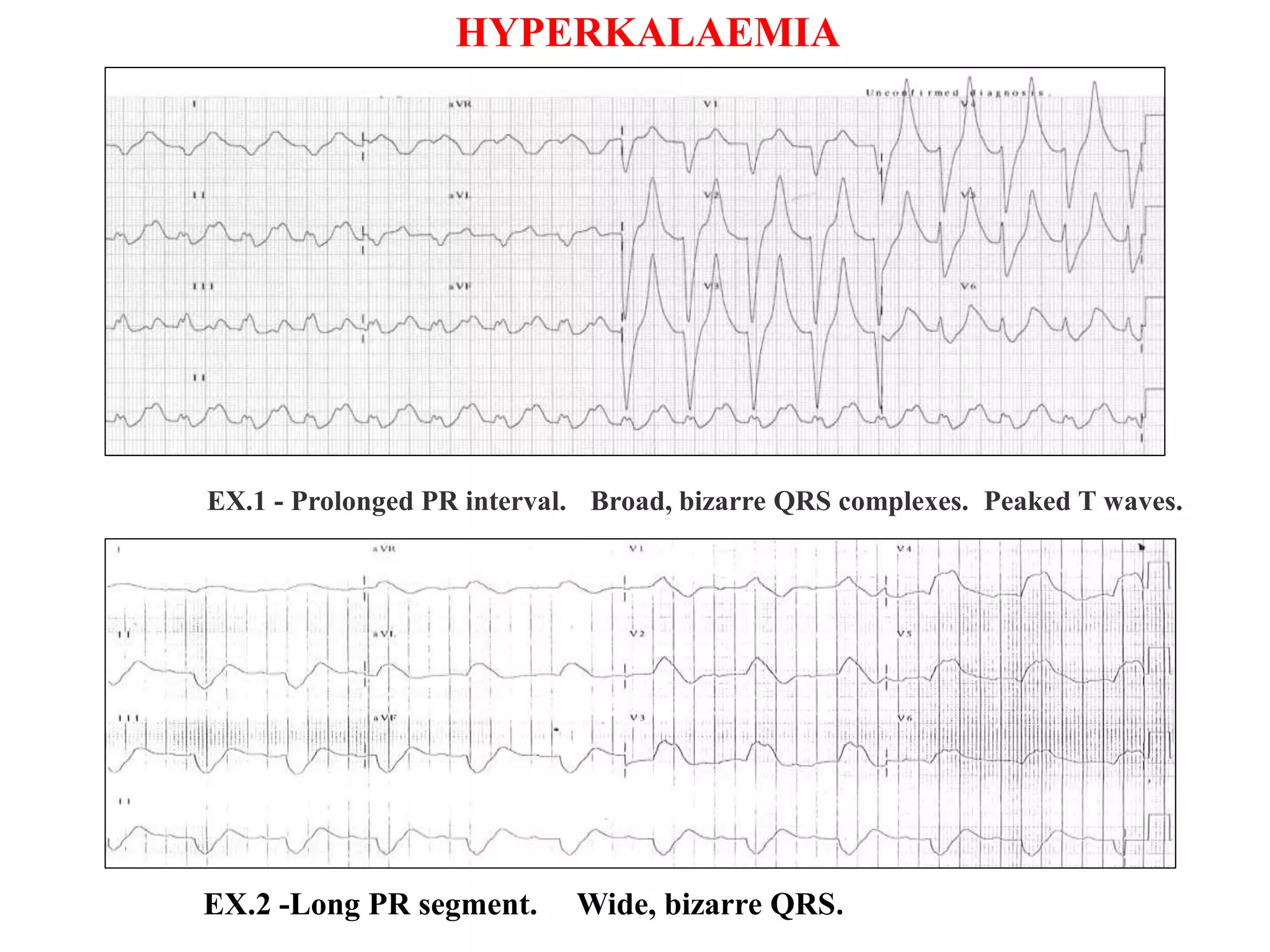





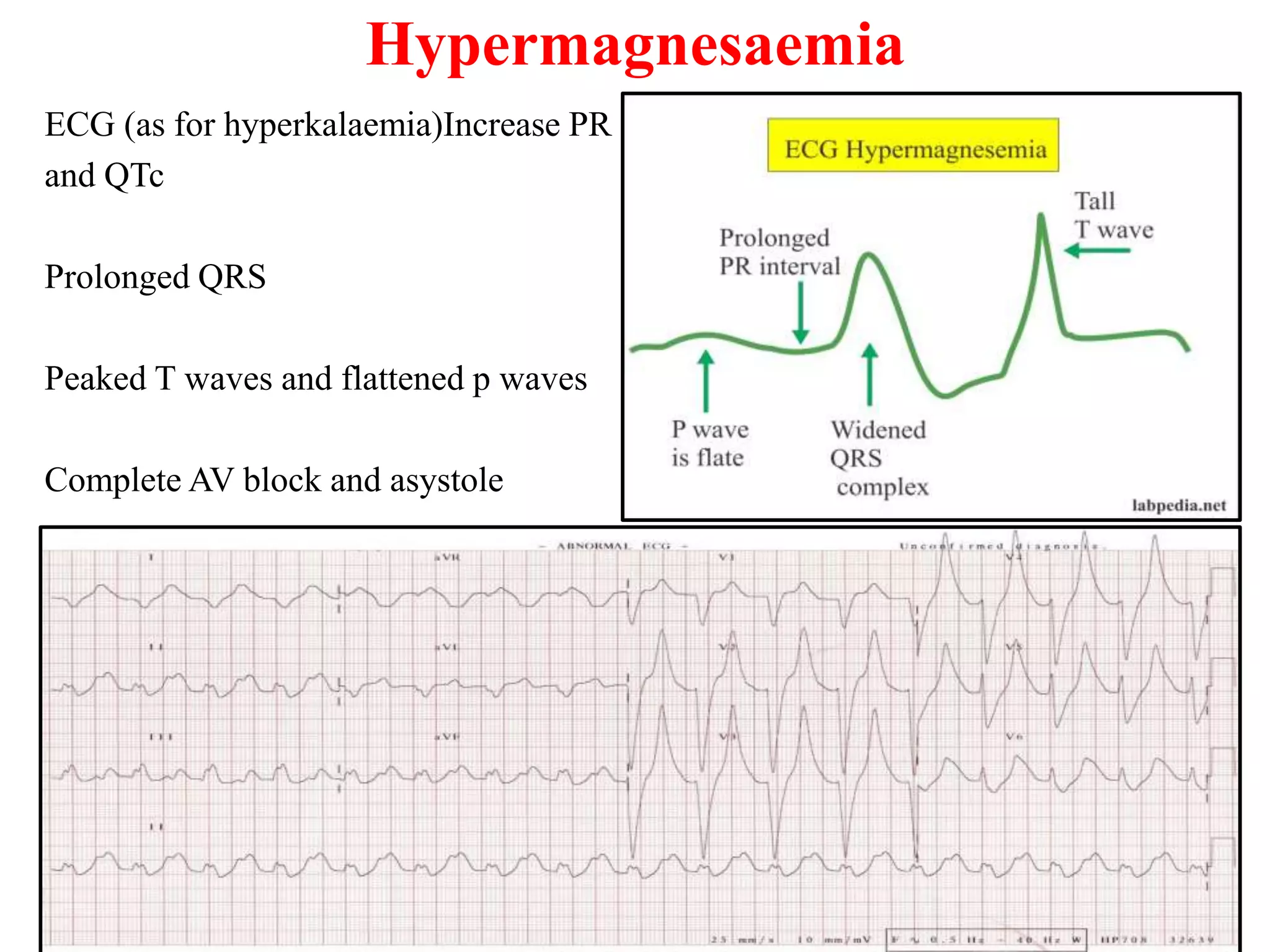


Hypothermia, hyperthermia, and various electrolyte abnormalities can cause characteristic ECG changes. Mild hypothermia (32-35°C) may cause sinus bradycardia or J waves, while severe hypothermia (<29°C) can prolong intervals and cause cardiac arrest. Hyperthermia (>37.5°C) may lead to sinus tachycardia or ST changes. Hyperkalemia causes peaked T waves, QRS widening, and higher levels can arrest the heart. Hypokalemia results in flattened T waves, prolonged QT, and may trigger dangerous rhythms.






































![Cardiology for g psaediatrics[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cardiologyforgpsaediatrics1-120611235613-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





































