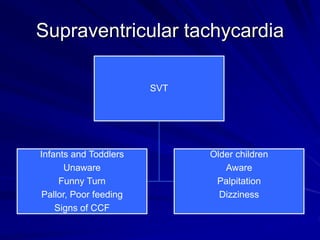
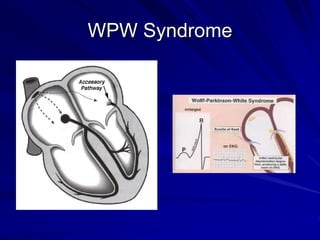
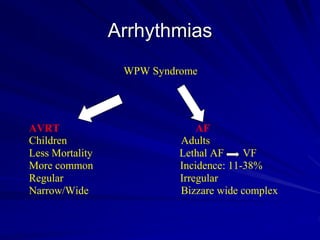
This document provides guidance on pediatric EKG interpretation. It discusses the key steps and aspects to analyze when reading a pediatric EKG, including rhythm, rate, QRS axis, intervals, hypertrophy, ST segments, T waves, and electrical heart diseases. Supraventricular tachycardia is highlighted as the most common tachyarrhythmia in childhood, with some cases being asymptomatic and others potentially leading to poor left ventricular function if not treated appropriately.