Downloaded 450 times
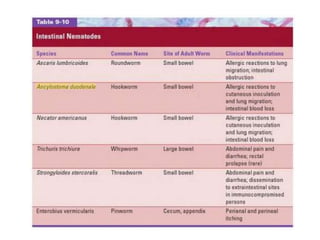
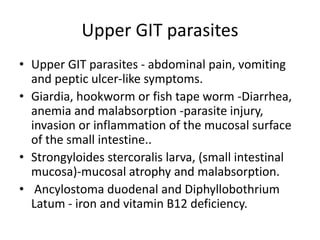

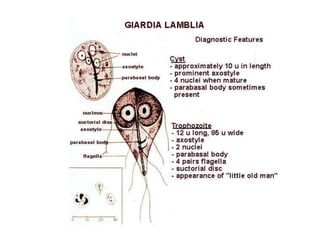
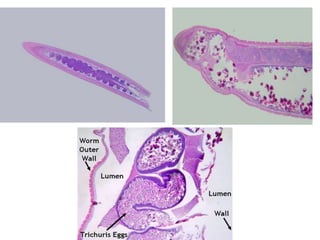
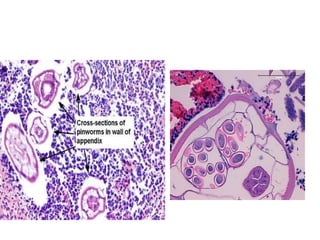
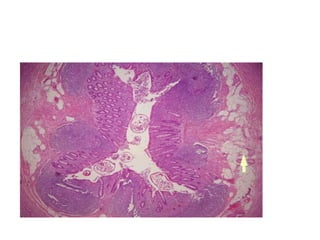
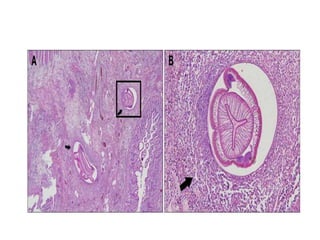
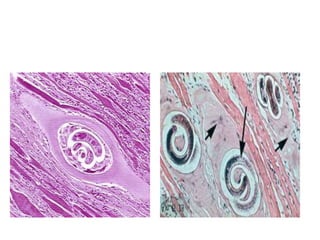





This document summarizes various intestinal and tissue parasites that can infect humans through contaminated food or water. It describes the clinical presentations, locations of infection, and histopathological findings for parasites such as Giardia lamblia, Strongyloides stercoralis, hookworm, Trichuris trichura, Cryptosporidium, Enterobius vermicularis, Entamoeba histolytica, Anisakis, Trichinella spiralis, Dracunculus medinensis, Schistosoma species, Echinococcus granulosus, Taenia saginata, cysticercosis, and filarial worms. Definitive diagnosis of many parasitic infections requires identification of eggs,























































































