Downloaded 25 times
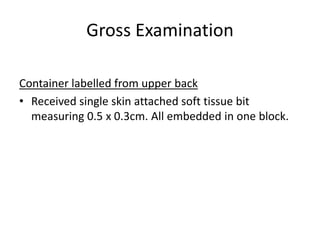
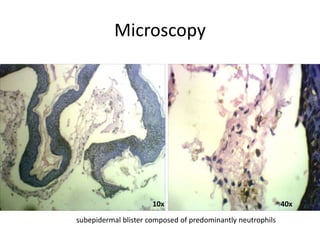
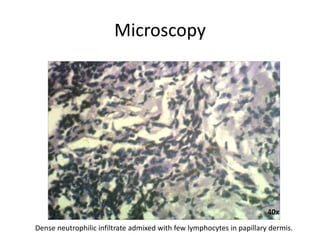
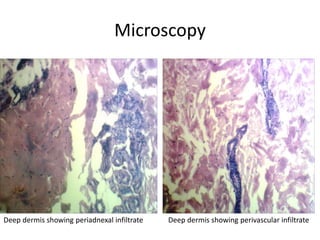
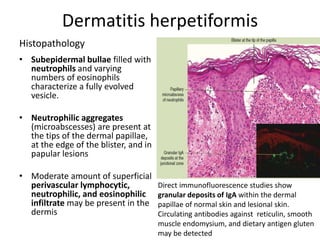
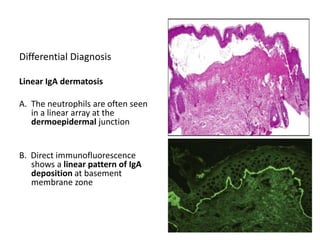
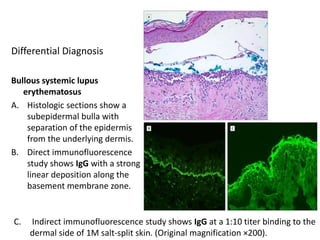
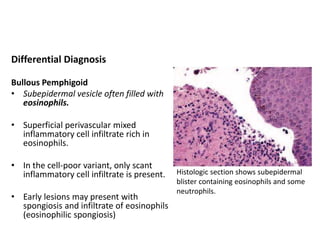
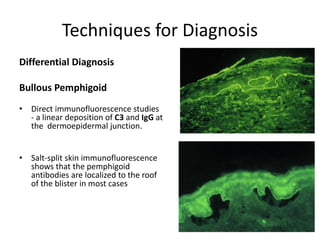
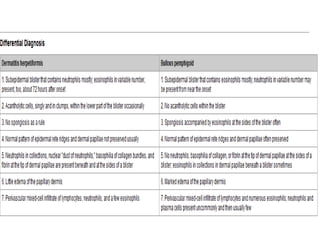

This document summarizes the histopathology findings of a skin biopsy from a 54-year-old female patient with a clinical diagnosis of bullous pemphigoid. Microscopy showed a subepidermal blister filled with neutrophils. There was a dense neutrophilic infiltrate in the papillary dermis. The impression was consistent with dermatitis herpetiformis. Further evaluation with direct immunofluorescence was advised to identify granular IgA deposits in the dermal papillae, confirming the diagnosis. Differential diagnoses including linear IgA dermatosis and bullous systemic lupus erythematosus were discussed.




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















