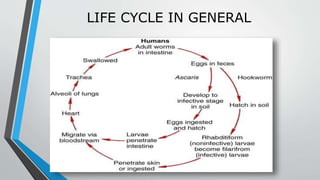
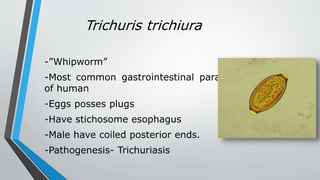
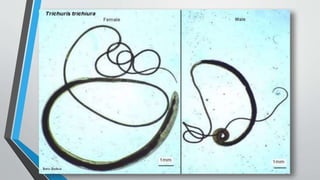
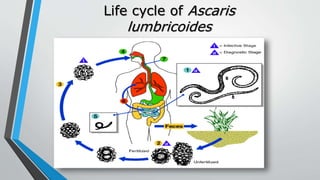
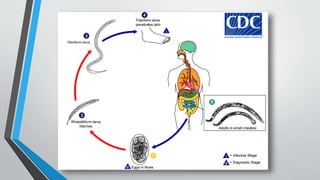
The document provides a comprehensive overview of nematodes, detailing their morphology, life cycle, and classification into classes Enoplea and Rhabditea. It specifically discusses the biology and pathogenicity of various species such as Trichuris trichiura (whipworm), Ascaris lumbricoides (roundworm), and Wuchereria bancrofti (causing lymphatic filariasis), including their interaction with hosts and symptoms of infection. Additionally, it covers diagnosis, treatment options, and preventive measures for nematode infections.