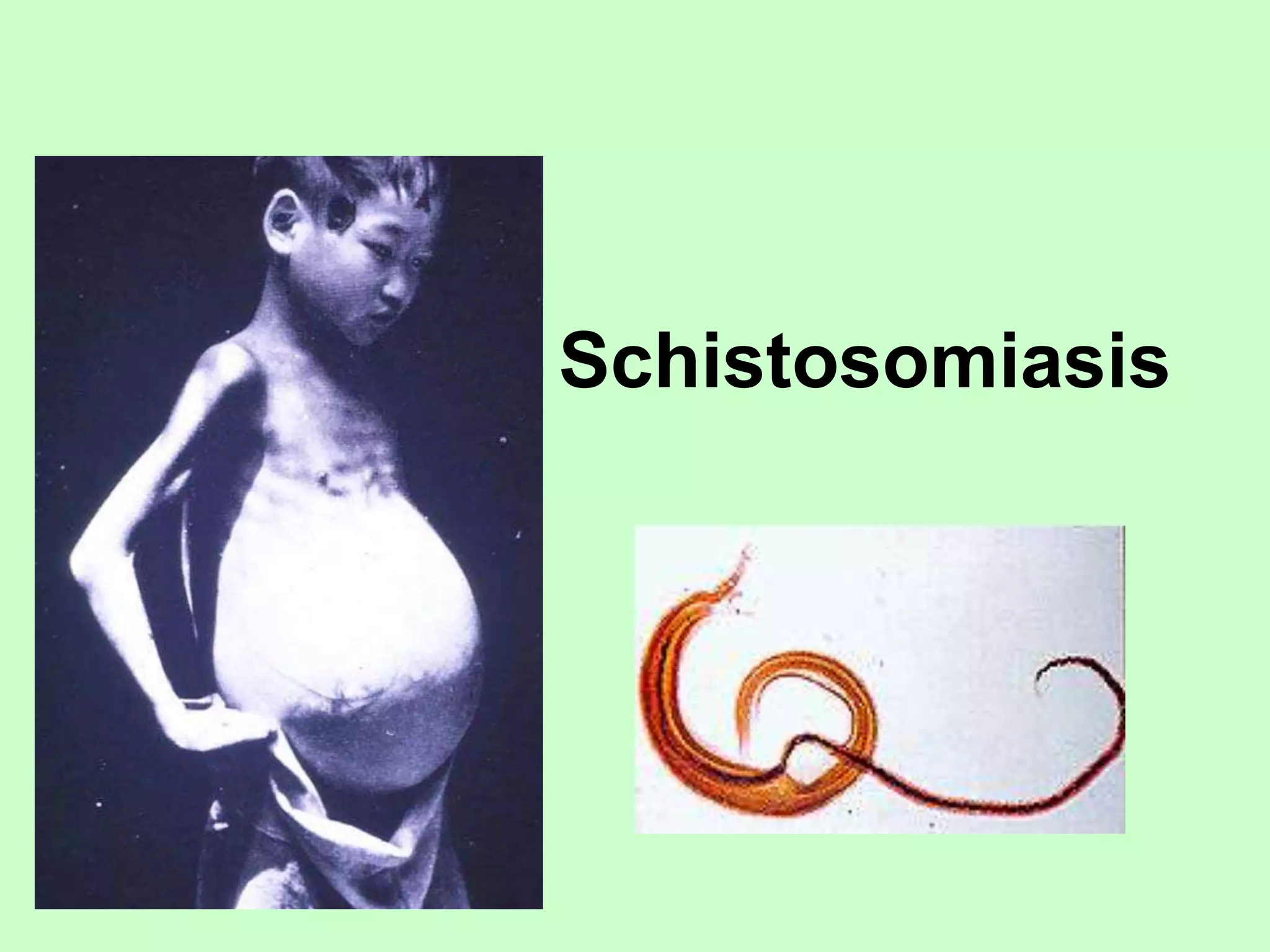
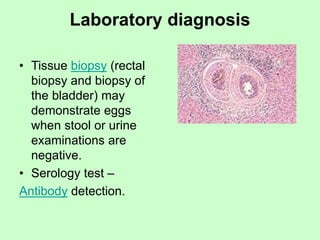
Schistosomiasis is a chronic parasitic disease caused by several species of flatworms. It is most commonly found in tropical and subtropical areas where contact with contaminated water can allow transmission from infected snails to humans. The parasites mature in the body and lay eggs that can cause damage to internal organs. Symptoms range from none to acute fever, rash, and organ damage depending on the parasite species and stage of infection. Diagnosis involves finding parasite eggs in stool, urine, or tissue samples. Treatment is with praziquantel which kills the parasites but does not prevent reinfection. Prevention relies on avoiding contact with contaminated freshwater in endemic areas.