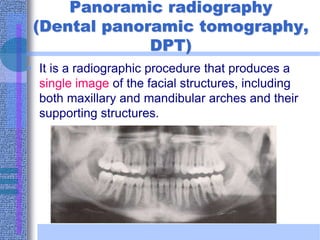
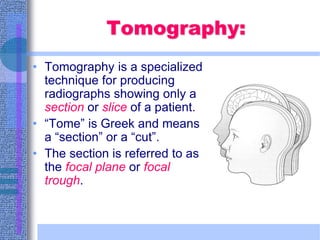
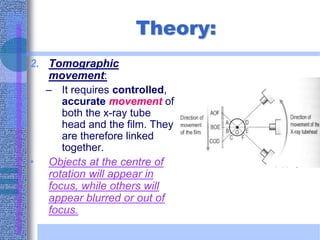
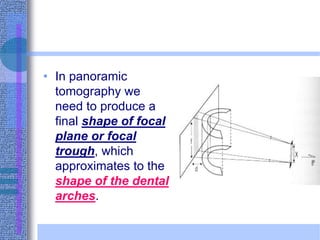
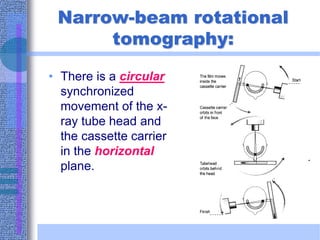
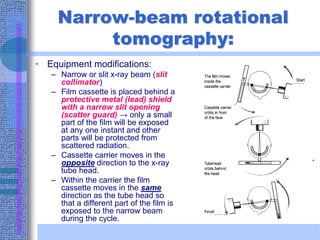
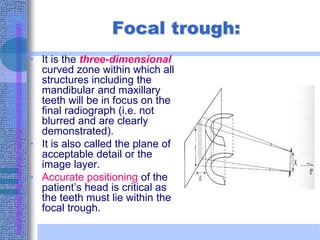
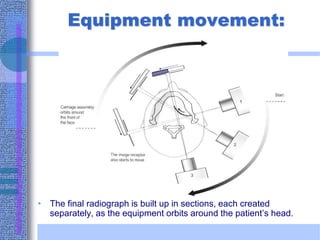
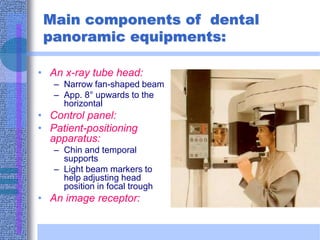
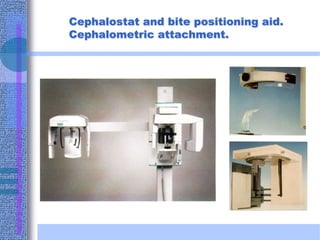
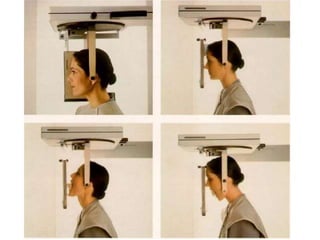
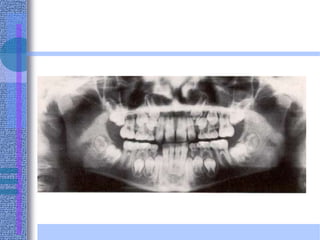
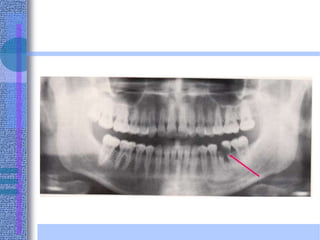
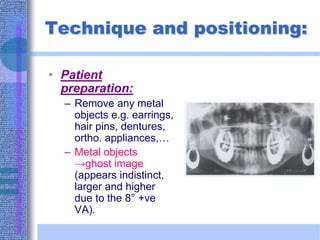
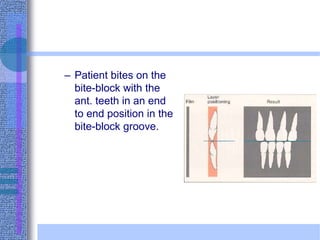
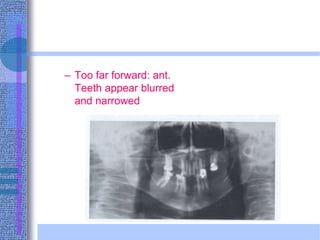
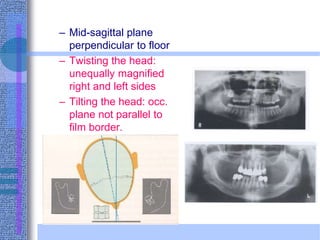
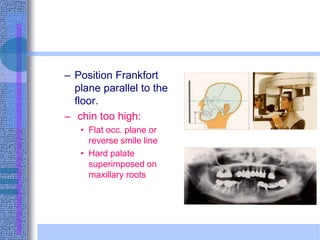
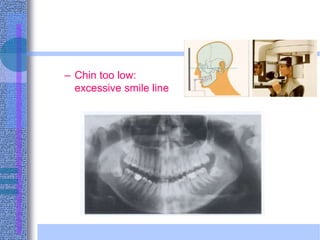
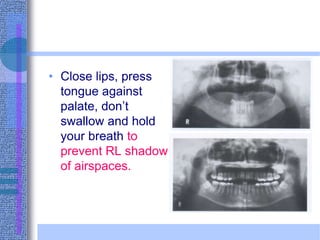
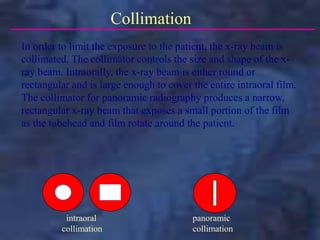
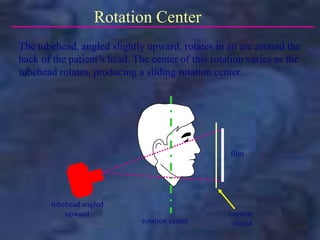
Panoramic radiography, also known as dental panoramic tomography (DPT), produces a single image of the facial structures including both dental arches. It utilizes a technique called tomography, which produces radiographs of a thin section or slice of the patient. In panoramic radiography, the x-ray tube and film rotate synchronously around the patient's head within a focal trough, producing multiple images that are merged into a single panoramic view. This provides visualization of teeth and jaws while minimizing radiation exposure compared to full mouth x-rays. Exact patient positioning is important for obtaining diagnostic quality images.