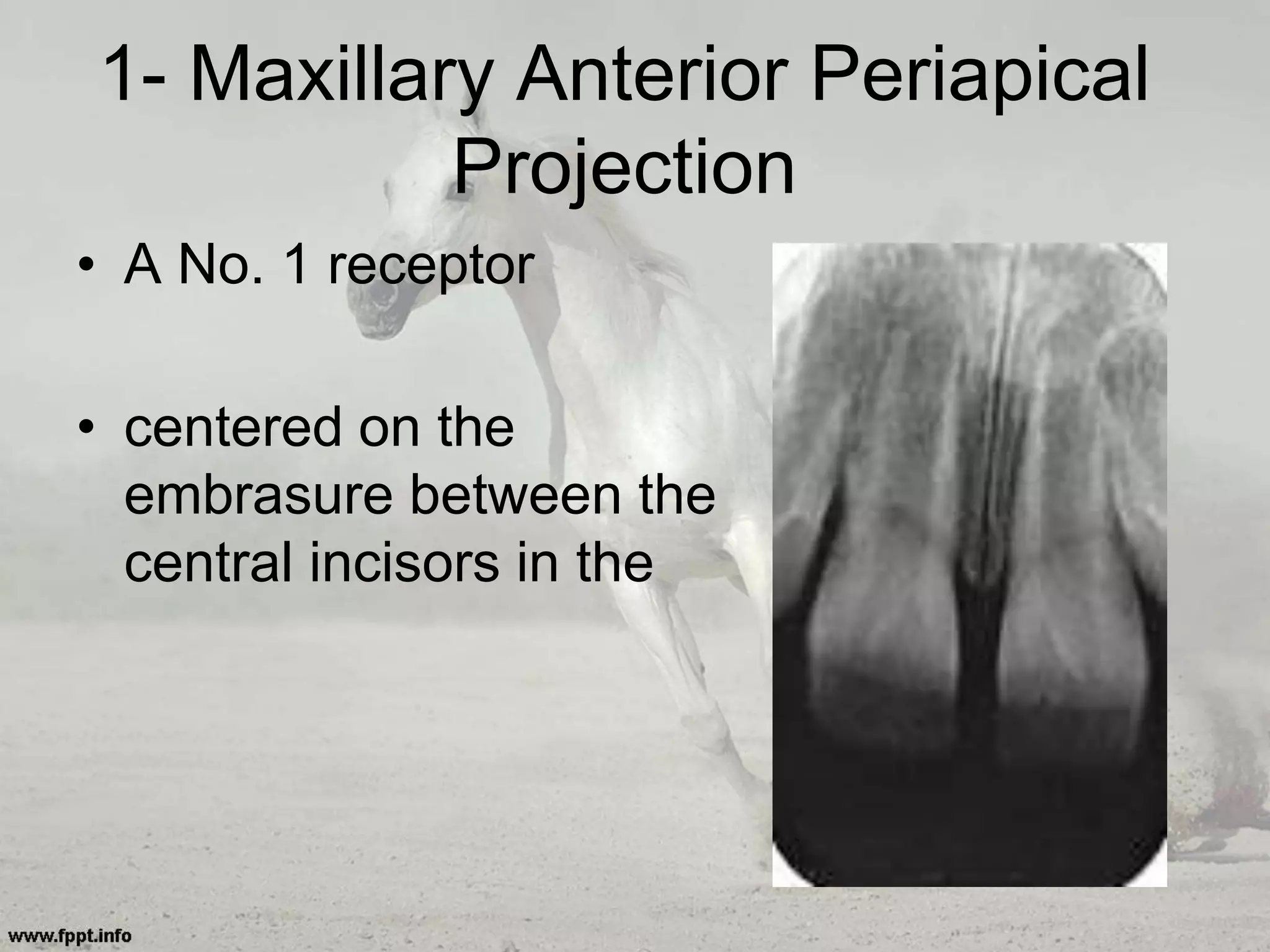
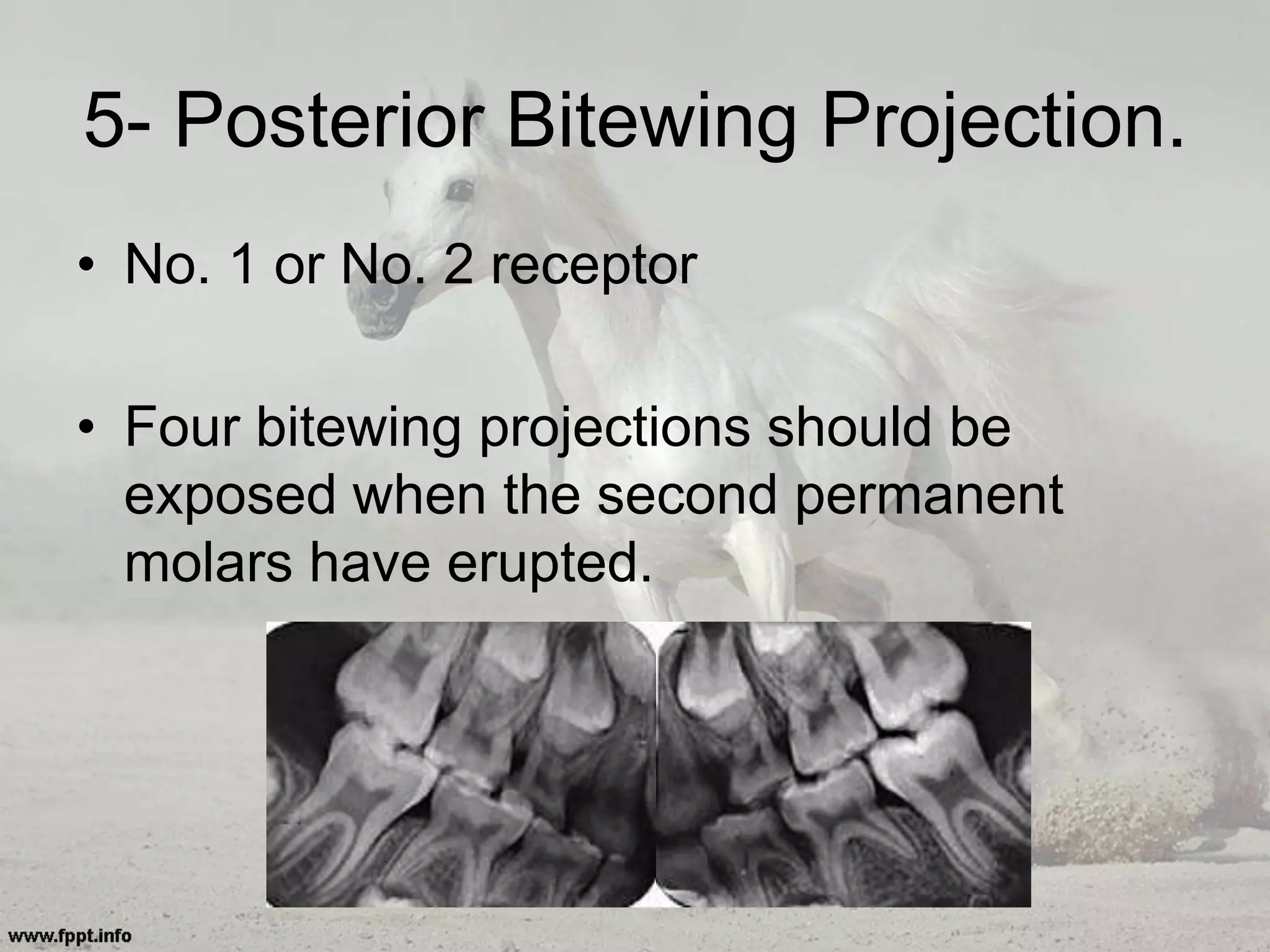
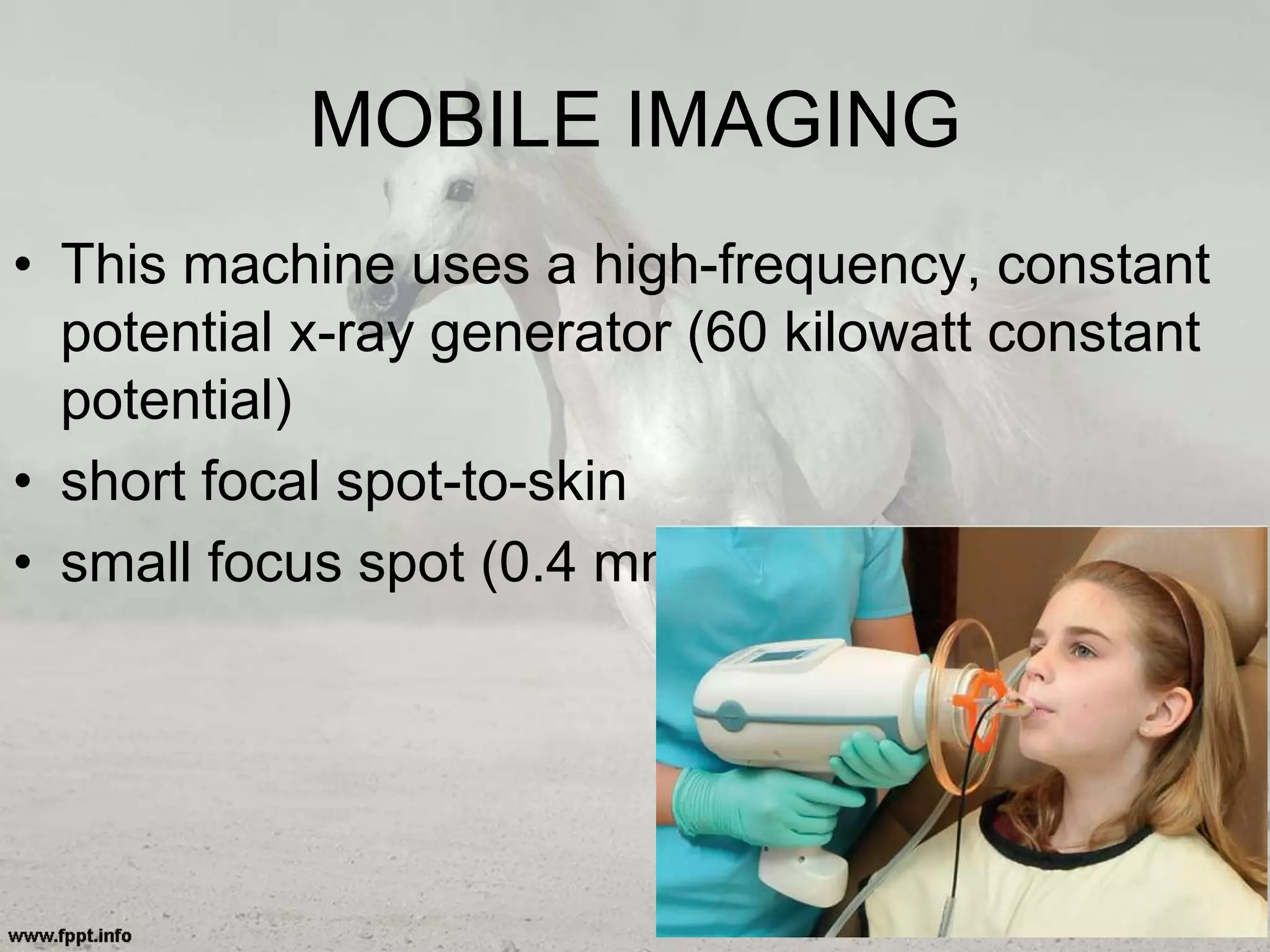
This document discusses intraoral radiography, categorizing images into periapical, bitewing, and occlusal projections. It details the criteria for quality radiographs, techniques for obtaining images using the paralleling and bisecting angle methods, and specific steps and angles for imaging various teeth. Additionally, it highlights the importance of proper receptor placement and central ray projection to minimize distortion and optimize clarity.