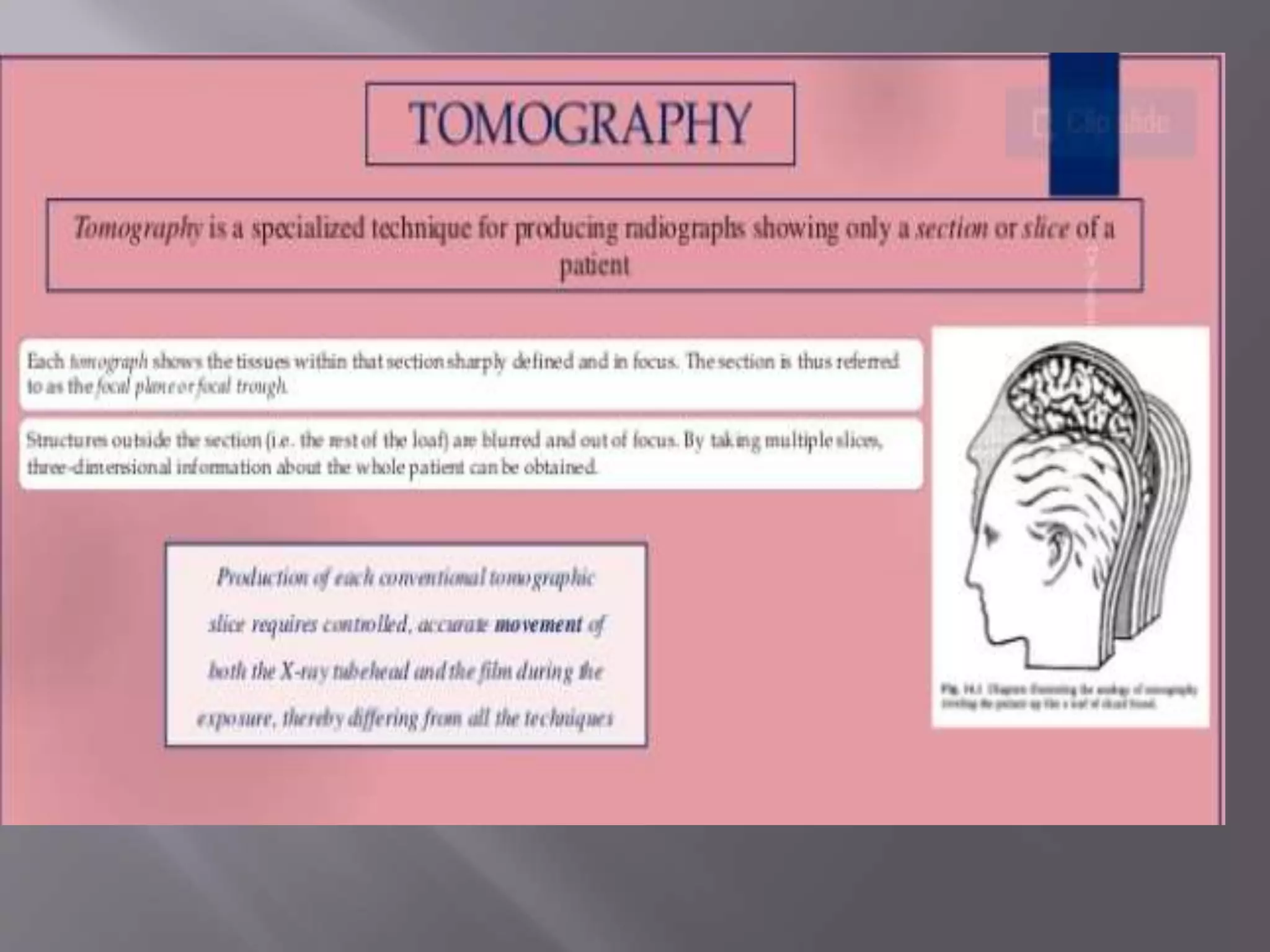
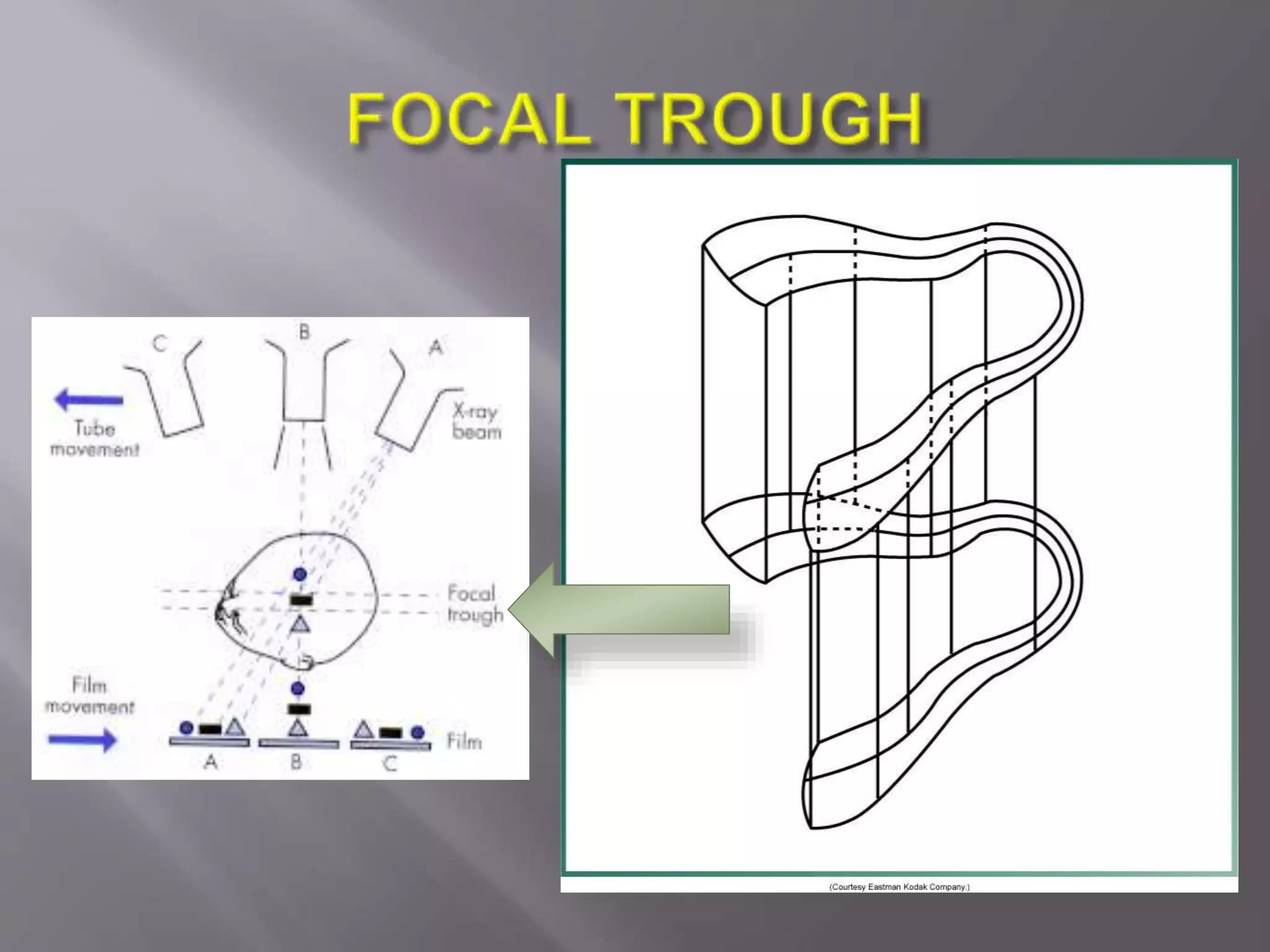
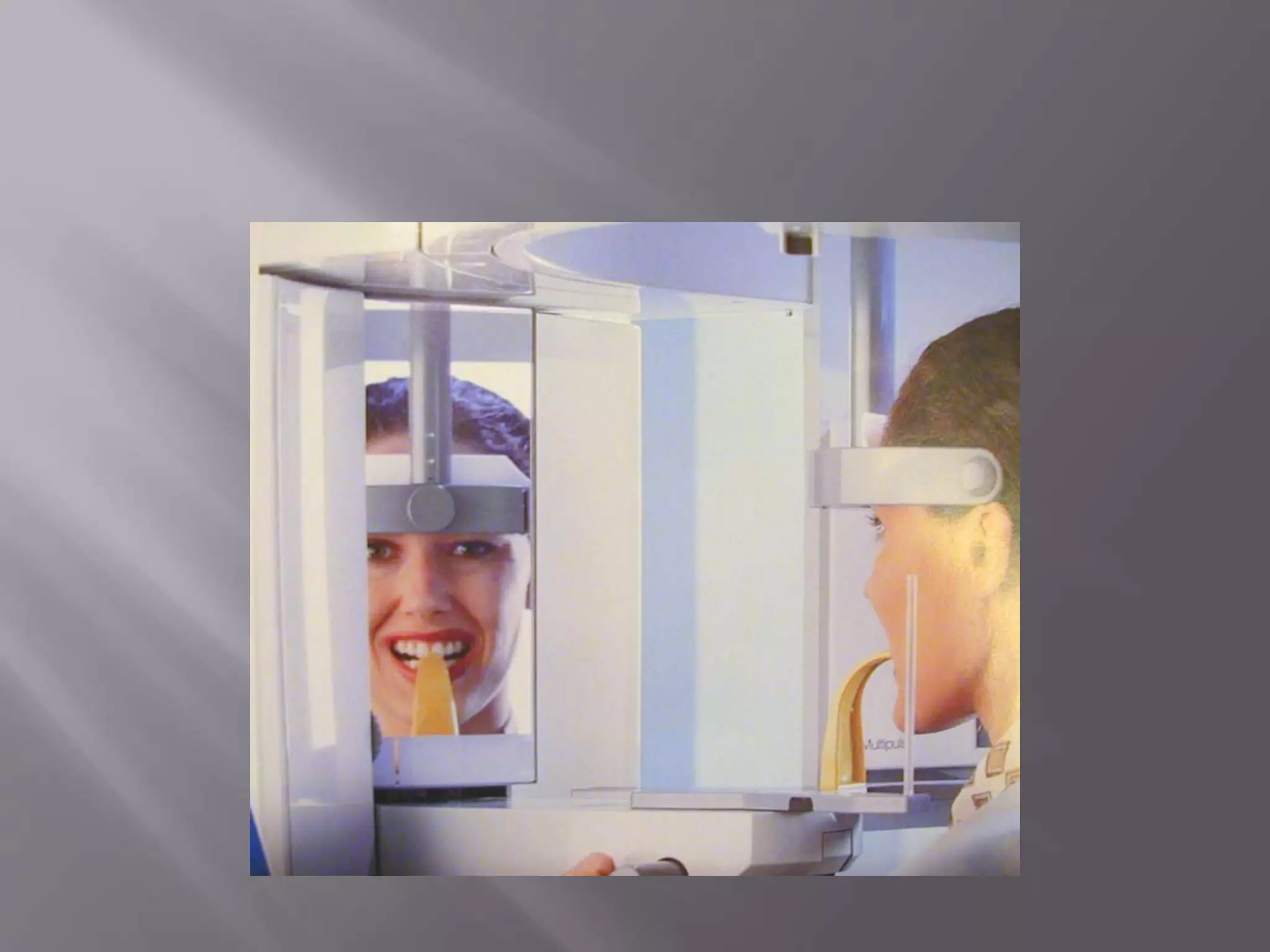
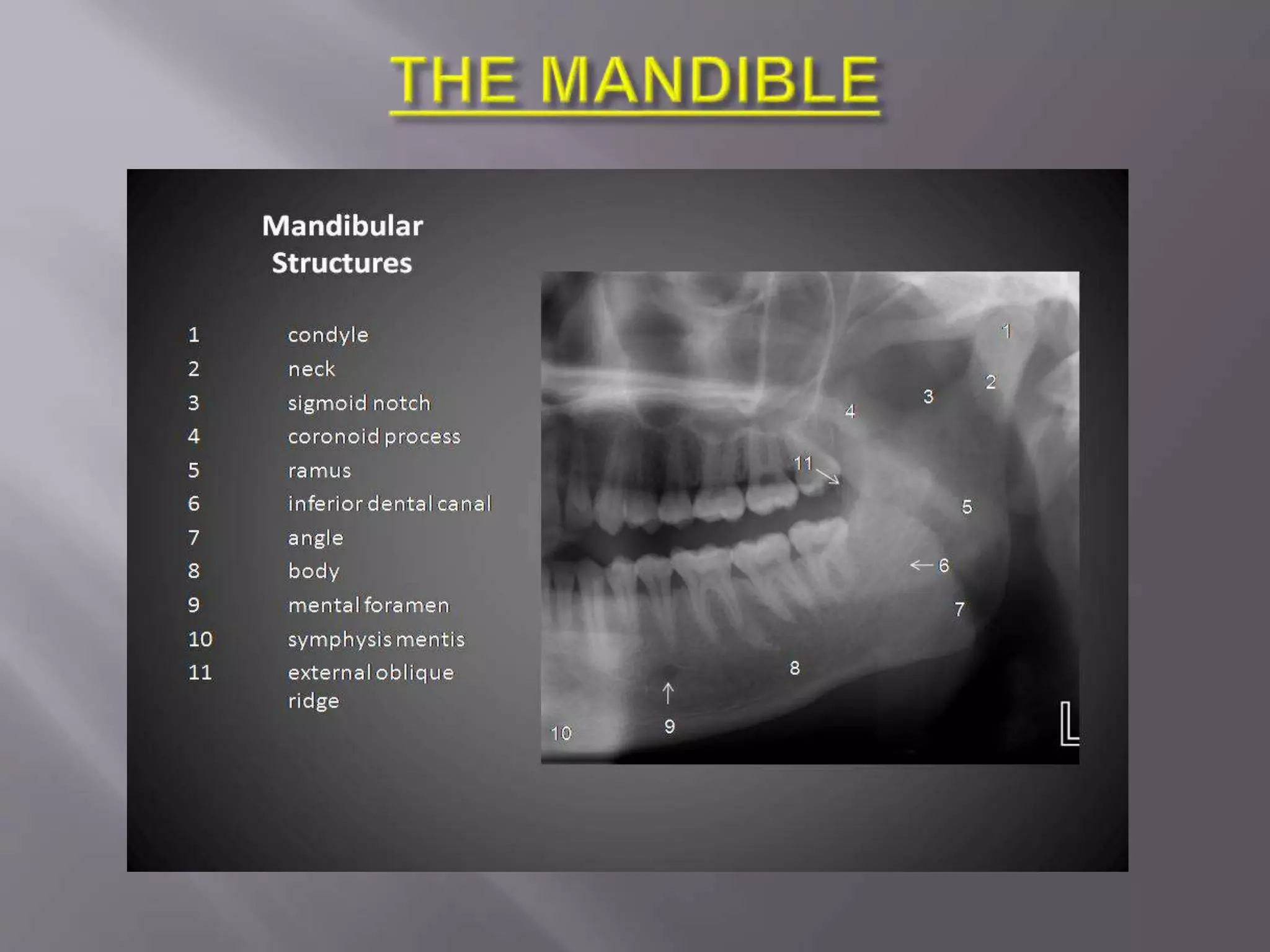
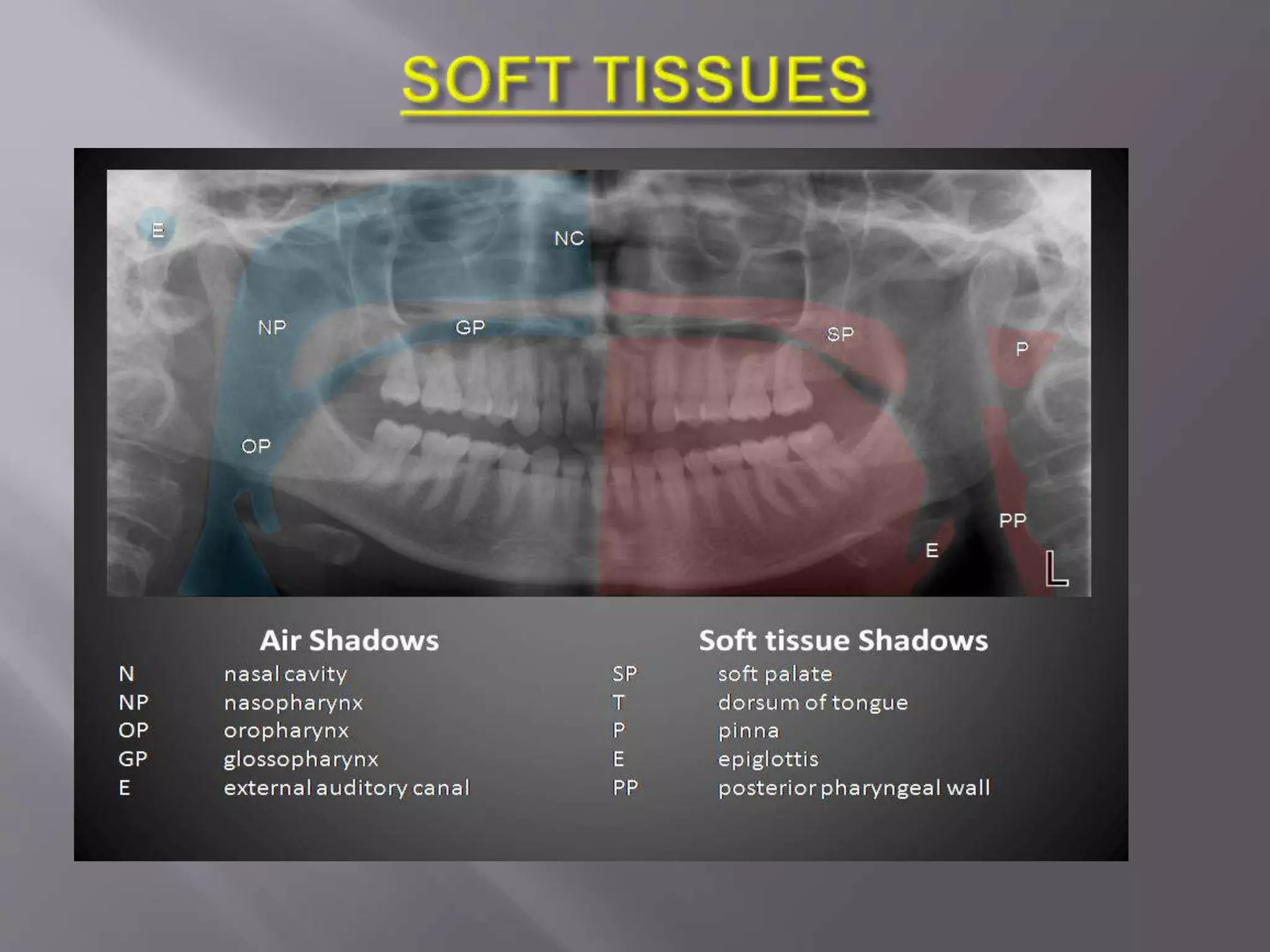
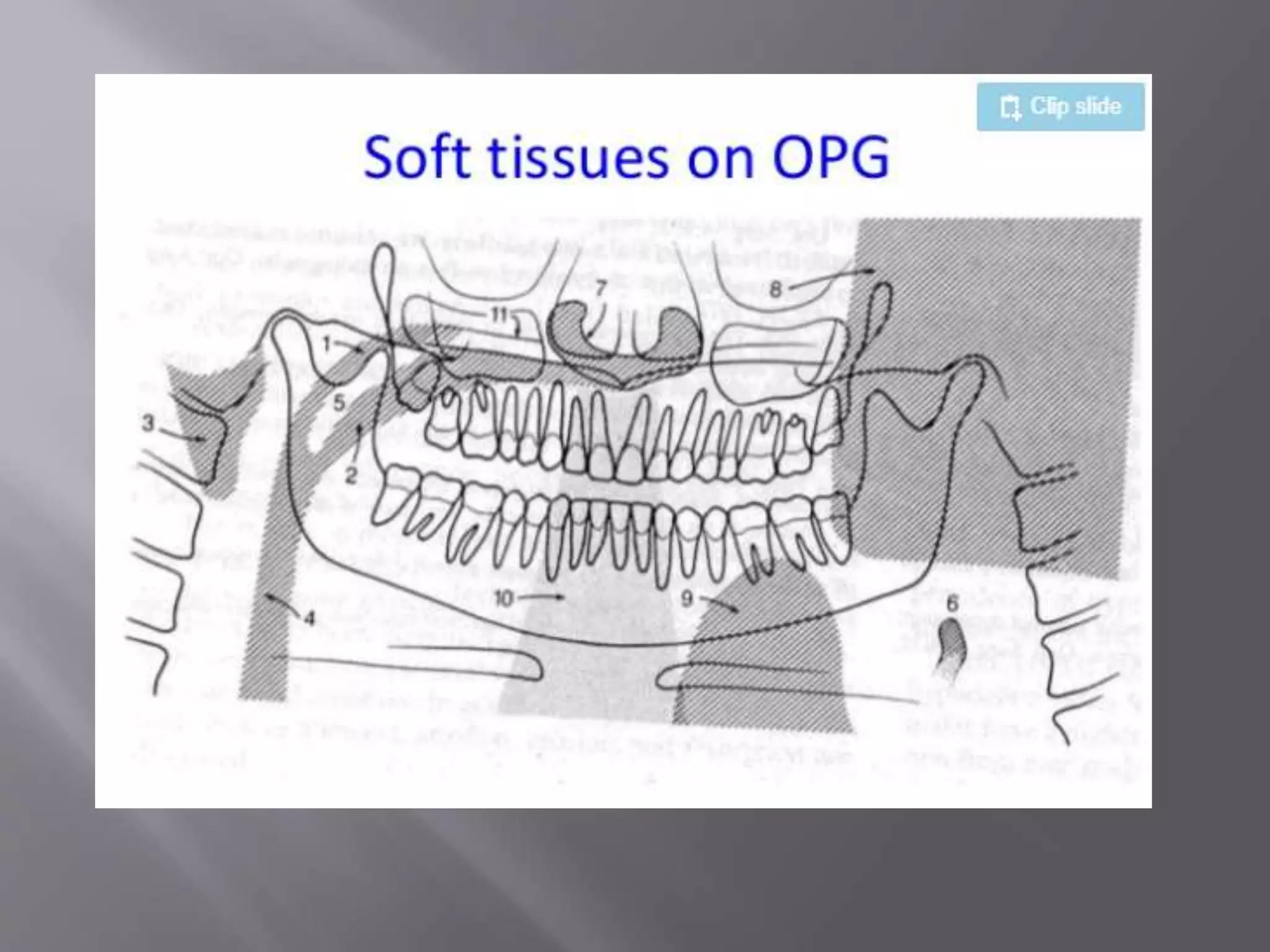
Panoramic imaging, also called pantomography, produces a single tomographic image of the maxillary and mandibular dental arches and their supporting structures. It is used to evaluate impacted teeth, eruption patterns, lesions, trauma, periodontal bone loss, and more. Panoramic imaging works by having an x-ray source and image receptor rotate around the patient's head, capturing structures within the focal trough sharply while blurring structures outside of it. Positioning the patient correctly is important for diagnostic image quality.





























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)















