Downloaded 13 times



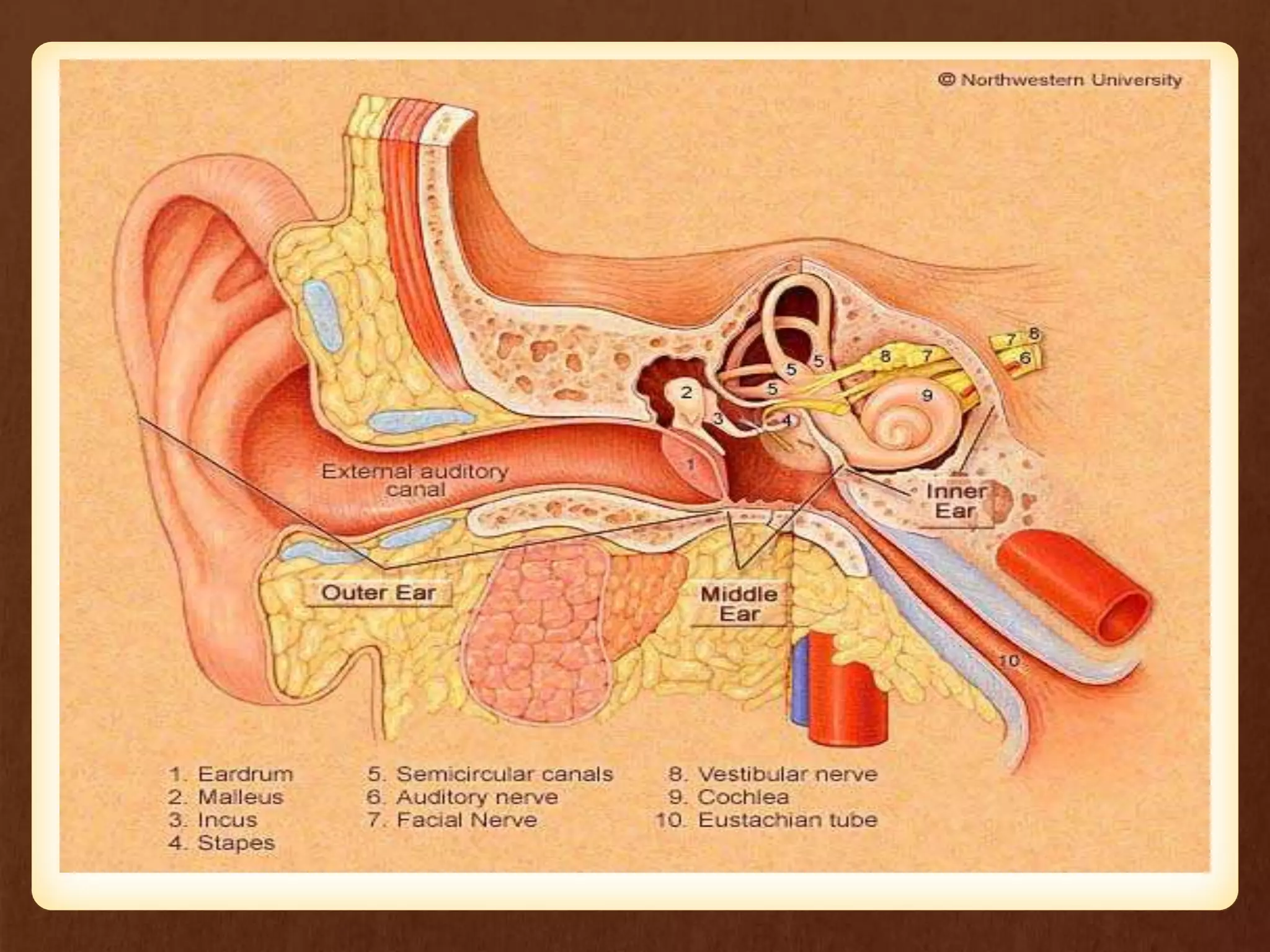























The document outlines the learning objectives related to otosclerosis, covering its definition, causes, pathophysiology, clinical manifestations, diagnostic measures, and management strategies. It highlights that otosclerosis leads to conductive or mixed hearing loss due to the abnormal bone growth around the stapes in the middle ear. The management includes both medical treatments and surgical interventions, with an emphasis on assessing the patient's condition, providing education, and ensuring follow-up care.























































































