Downloaded 21 times




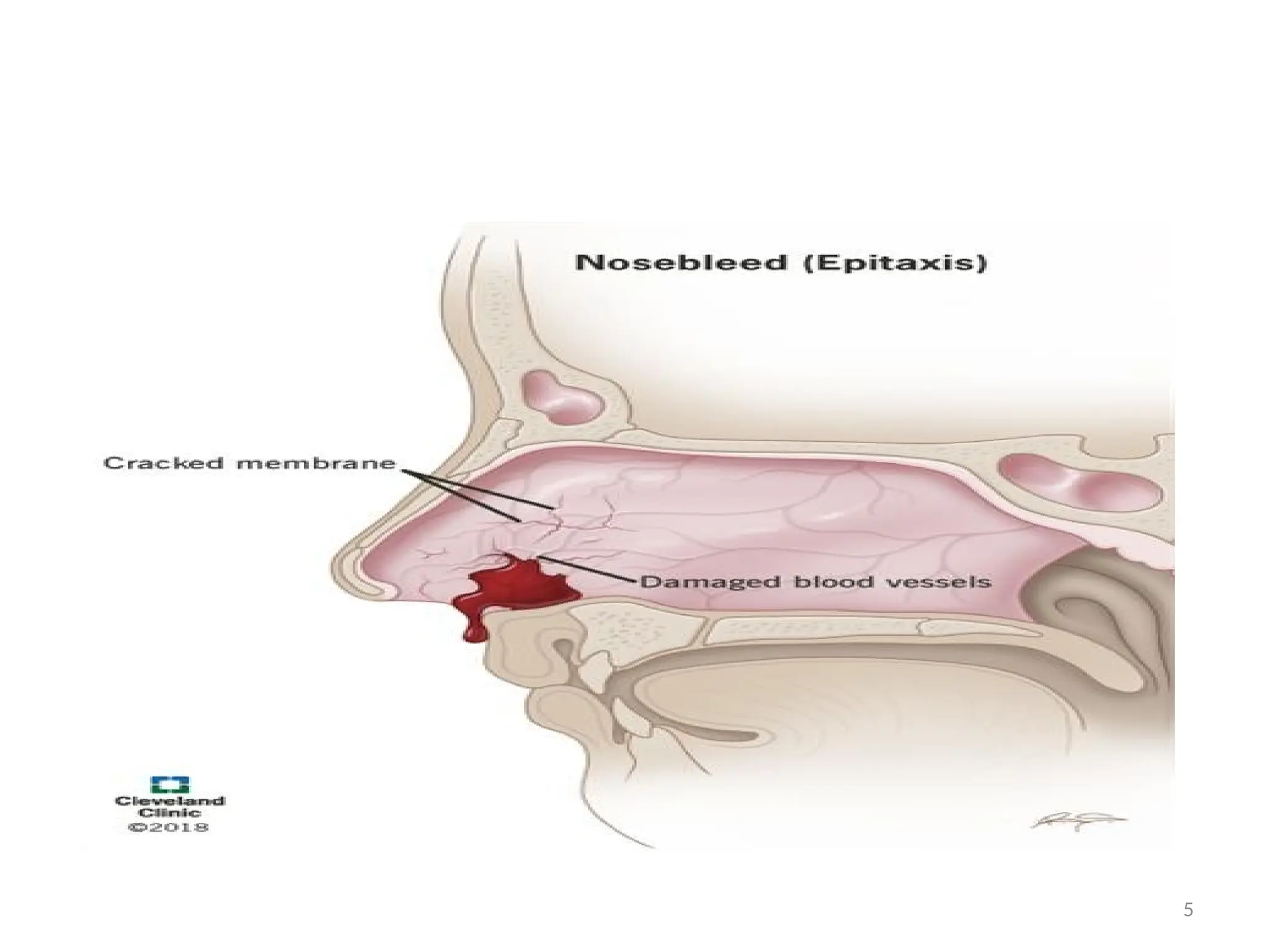
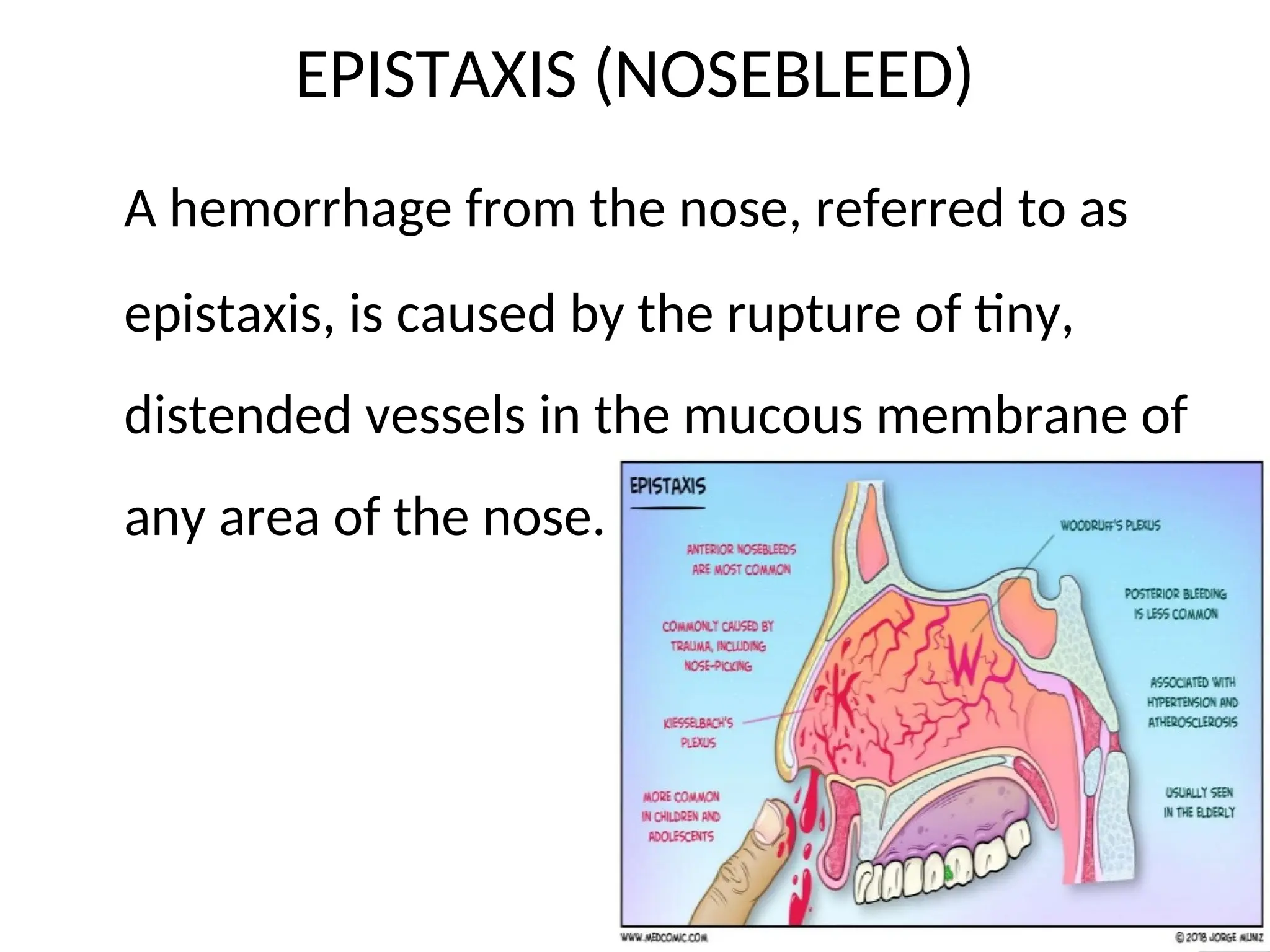







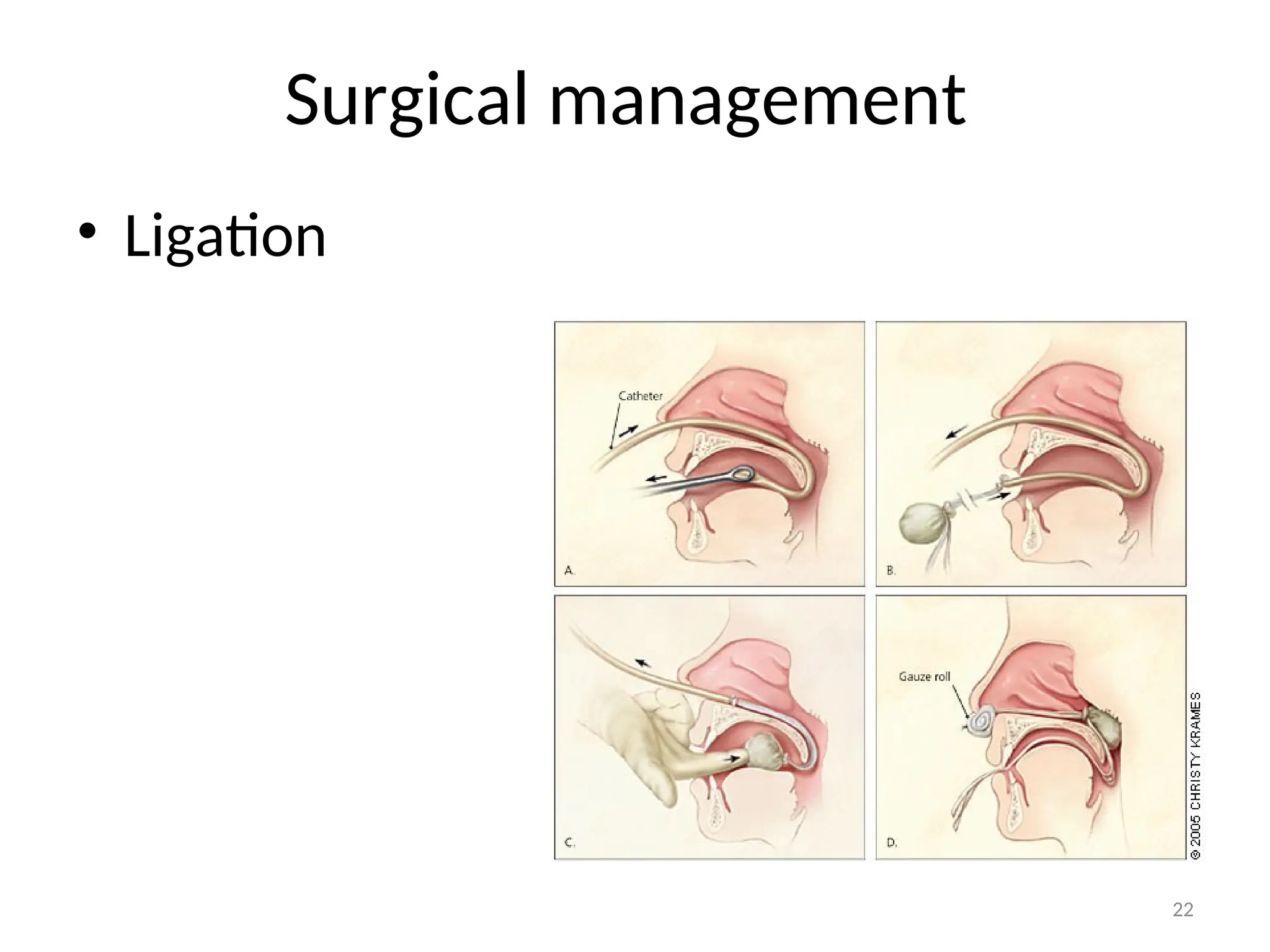



This document outlines the educational objectives related to epistaxis, including its definition, causes, clinical manifestations, and management strategies. Epistaxis, or nosebleed, commonly arises from the anterior nasal cavity due to ruptured blood vessels and can be categorized into anterior and posterior types. Management involves re-establishing hemostasis through various medical and nursing interventions, including pressure application, medication, and, if necessary, surgical procedures.























































































