Download to read offline
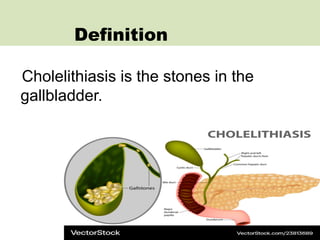
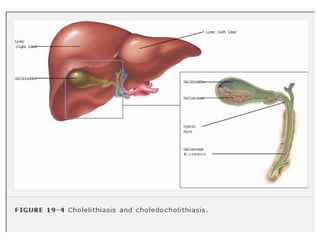
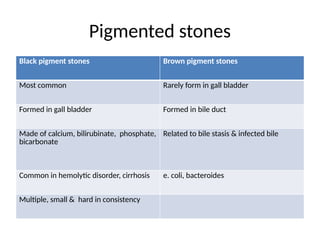
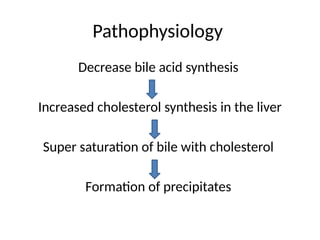
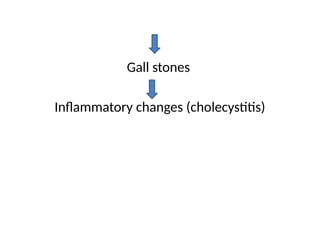
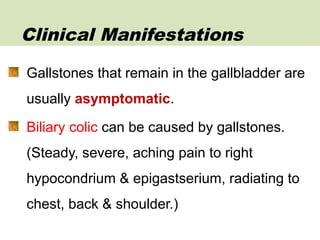

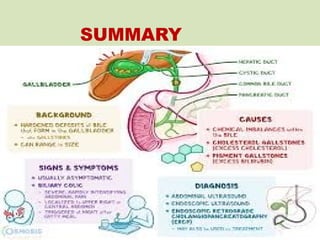


The document provides an overview of cholelithiasis, detailing its definition, etiology, risk factors, clinical manifestations, and management strategies. It emphasizes the significance of gallstones as a common health issue in India, alongside the diagnostic evaluation and potential complications arising from the condition. The text also outlines nursing assessments and health education pertinent to patients with cholelithiasis.