Downloaded 15 times

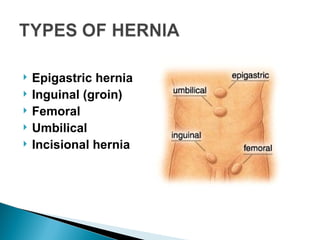

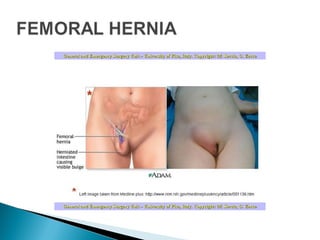


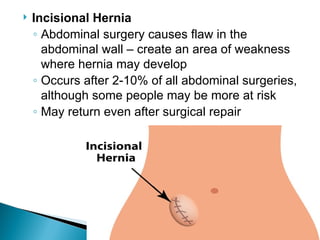

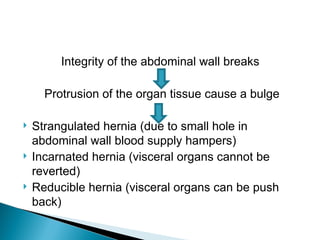



The document outlines hernias, abnormal protrusions of body parts, detailing their types, causes, symptoms, diagnoses, and treatments. Abdominal wall hernias are prevalent, especially inguinal hernias, which comprise 75% of cases. The text also addresses nursing considerations regarding preoperative and postoperative care for patients with hernias.
















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






