
Downloaded 189 times
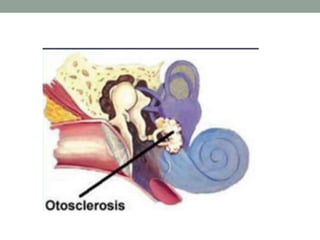
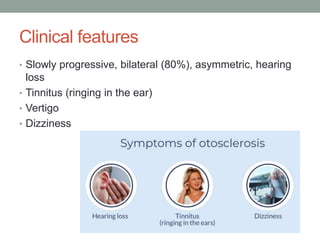
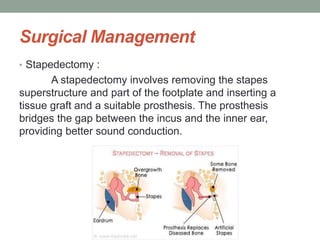
Otosclerosis is a disease characterized by abnormal bone growth in the middle ear that causes hearing loss. It is caused by bone remodeling that fixes the stapes bone, preventing sound vibration. Symptoms include progressive, asymmetric conductive hearing loss, tinnitus, and dizziness. Diagnosis involves audiogram and physical exam. Treatment options include hearing aids, sodium fluoride to arrest progression, and stapedectomy or stapedotomy surgery to restore hearing. Post-operative care involves rest and avoiding pressure changes or water entry into the ear during healing.

















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


